Non-Vascularised Ipsilateral Fibular strut – A Modality to Treat Giant cell tumor of lower end radius using Anterior Approach.
Vol 1 | Issue 1 | May – August 2015 | page:45-47 | Ninad Godghate[1], Vikram V Kadu[1], K A Saindane[1], Neha N Godghate[1].
Author: Ninad Godghate[1], Vikram V Kadu[1], K A Saindane[1], Neha N Godghate[1].
[1]ACPM Medical College, Dhule – 424001, Maharashtra, India
Address of Correspondence
Dr. Vikram V. Kadu
ACPM Medical College, Dhule – 424001, Maharashtra India
Email : vikram1065@gmail.com
Abstract
Introduction: Giant cell tumor is a benign bone tumor, locally aggressive with low malignant potential. The goal of treatment of this tumor at the distal radius is complete removal of the tumor and reconstruction of the bone defect in order to preserve maximum function of the wrist joint.
Case Series: This is a retrospective study conducted in 5 consecutive patients of GCT of distal radius. All patients presented with pain and swelling over distal end radius and were assessed clinically and radiographically. X-ray showed lytic lesion at lower end of radius suggestive of GCT. Histopathological examination and FNAC was done to confirm the diagnosis. Once the patient was fit for Surgery, wide excision of tumor and reconstruction with ipsilateral non-vascularised proximal fibula was performed. DCP plating was done to secure the fibular graft to the radius. 2 K – wires, 1 transverse through the fibula and ulna and 1 through fibula into the carpals were used for additional fixation and to help maintain the fibula and ulna in close approximation.
Results: At final follow up of minimum 1 year, all cases had good graft union with no recurrence. The range of motion of the wrist was near normal with no instability and good grip strength. Although this is an early follow up no graft collapse and no arthritic changes were noted. There were no complications both at donor and recipient graft sites.
Conclusion: Autogenous non-vascularised fibular graft for reconstruction of distal radius GCTcan be considered as a reasonable option for treating such conditions. Long term follow up will be needed to assess temporal complications and long term survival of the graft.
Keywords: Distal radius, fibula, GCT, ipsilateral.
Introduction
Juxta-articular giant cell tumors of the lower end radius are common and present a special problem of reconstruction after tumor excision. Various reconstructive procedures described, non-vascularised fibular autograft has been widely used with satisfactory functional results. Giant cell tumors (GCT) of the bone are aggressive and are recognised for variable clinical behaviour, which is not always related to radiographic or histological appearance [1]. Complete excision of the tumor offers the best chance of cure but sacrifices the articular surface and presents complex reconstructive problems. Giant cell tumor (GCT) of bone is a benign but locally aggressive tumor with tendency for local recurrence [2]. Distal radius is the third most commonly involved site of skeletal GCTs (10% cases) next to distal femur and proximal tibia [3,4]. Goals of treatment are to achieve satisfactory removal of the tumor, lessen the chance of local recurrence and to preserve as much wrist function as possible.
Case Series
This is a retrospective study conducted between 2004-2014. We studied 5 consecutive cases of GCT involving the distal radius operated by en-bloc resection of tumor followed by reconstruction with ipsilateral non-vascularized fibular graft with a minimum 1 year follow-up. Informed consent from the patient was taken and approval from the institutional review board was obtained for the study. Of the 5 cases studied, 3 were males and 2 were females. 3 right sided and 2 left sided. Mean age group was 22 yrs (14 – 30 yrs). Campanacci’s staging system for giant cell tumour of the bone [5] was used for cortical breach. According to this system, 2 tumours were classified as Stage I and 3 tumours as Stage II. Once the patient was medically fit, surgery (ORIF with resection of distal end of radius and reconstruction with ipsilateral non vascularised proximal fibula along with plate and 2 k-wires) was performed.
Surgical Technique
Patient supine on the operating table, with the arm on an arm board. Tourniquet on the arm was applied without exsanguinating the limb. Incision taken from the distal flexor crease of the wrist proximally upwards. The plane between the brachioradialis and flexor carpi radialis longus was used to reach upto the bone. The distal end of the radius was resected and measured. According to the measurement, the ipsilateral proximal fibula was resected and was reconstructed after giving thorough wash to the reconstruction site. The fibula was then fixed to the radius with a 6 hole DCP plate and 2 transverse k-wires at the distal end to stabilize the distal DRUJ. The path of common peroneal nerve was encased in soft tissue which was attached to proximal tibia. Closure was done and drain was kept. Below elbow slab was provided post-operatively.
Case Study
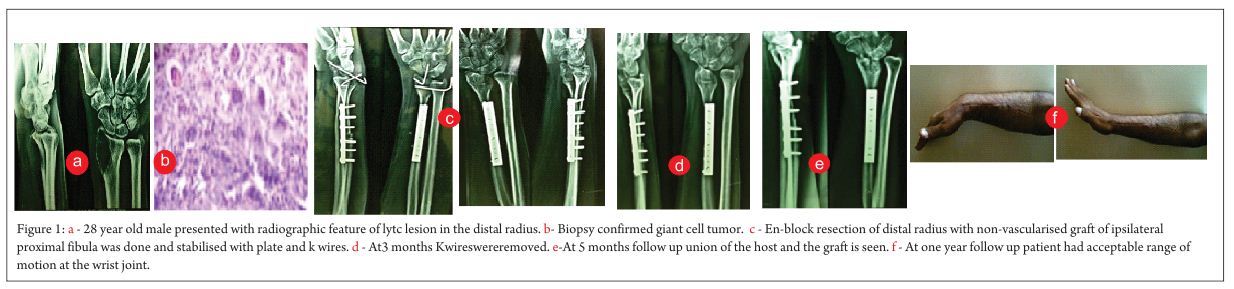
28 yrs old male presented to our OPD with complaints of pain and swelling over distal radius, moreover on the lateral side since 3 months. The swelling was initially small (Pea shaped) and gradually increased. On clinical examination, skin over the swelling was normal, swelling was diffuse and was fixed to the bone. The movements at the wrist joint was painless but the patient had tenderness on deep palpation. The egg shell crackling sign was absent on palpation. X-ray (Fig 1a) showed lytic lesion at the distal end of the radius. It was characteristic of soap bubble appearance. FNAC was done which revealed GCT. Further histopathology (Fig 1b) was done which confirmed GCT. Once the patient was medically fit, surgery (ORIF with resection of distal end of radius (Fig 1c) and reconstruction with ipsilateral non-vascularised proximal fibula along with plate and 2 k-wires) was performed. 6 hole DCP plate was used for reconstruction of the fibula to radius and 2 k-wires for additional stability to distal radio-ulnar joint. The patient was given below elbow slab post-operatively for 4 weeks and then below elbow cast for another 2 months. The arm was protected in corset for 1 yr. The 2 k-wires were removed at 3 months follow-up (Fig 1d). At 5 months follow-up (Fig 1e), patient was clinically and radiologically assessed and physiotherapy was started. At 1 yr follow-up (Fig 1f), The patient had gained acceptable range of movement with excellent grip strength, without any complication and returned to his previous work. All patients completed one year follow up and were called for final assessment. Bone graft had united in all cases with acceptable range of motion when compared to opposite side. There were no obvious complications, arthritis or recurrence.
Discussion
Giant cell tumor is an aggressive lesion with a high rate of recurrence [6]. There are reports that giant cell tumors in the lower end of the radius are more aggressive and metastasize more often to the lungs(1). Non-vascularised fibular autograft was first used in 1945 for congenital absence of radius(7). Later, fibular transplants were used by various authors for tumours of the lower end radius(8). This reconstruction technique has yielded good functional results for giant cell tumour of the lower end of the radius in various series, although large series with longer follow-ups are few(9).
In our study, we treated 5 patients with giant cell tumour of the distal radius by resection and ipsilateral non-vascularised fibular graft. Non-vascularised proximal fibular graft is reasonably congruous with distal radius and incorporated more rapidly. The graft is easily accessible without donor site morbidity. No allograft was used in our study. The patients we studied belonged to young generation in which limb salvage along with functional range of motion is the demand. The aim of treatment is to remove the tumor, reduce the chances of recurrence and preserve the joint function.
Resection of distal radius and reconstruction with ipsilateral non-vascularized fibula offers several advantages like more congruency of carpal joint, rapid incorporation as autograft and easy accessibility without significant donor site morbidity. Structural change is also minimal. Moreover, immunogenic reactions are absent. Case reports of joint preservation using vascularized fibula or prosthesis are found to be few and inconclusive(10,11]. Vascularised fibula has advantages of speeding up the healing time and early mobilization but at the same time its disadvantages includes; prolonged surgery time, need to sacrifice the arteries, skilled surgeon, not possible by an average orthopaedic surgeon.
The most commonly encountered complication in such cases are non-union, delayed union, wrist joint subluxation, subluxation of DRUJ. In our study we didn’t encounter any of the complications. Moreover, reconstruction with ipsilateral non-vascularised fibular graft is less time consuming, comparatively easy, can be done by any average orthopaedic surgeon and does not require any microvascular surgery. A proper length of fibular graft is a must to maintain the radial height and to prevent subluxation of the wrist joint. We ensured this by harvesting the fibula 2-3 mm more than the required length, which is the resected tumor length plus the safe margin. This 2-3 mm allowed us to achieve compression at the host-graft junction during fixation with DCP. A longer fibular graft will lead to subluxation of the wrist whereas 2 k-wires fixed in the distal fibula-ulnar joint further helps in stabilization of the wrist joint. There is a chance of stiffness of the wrist with relatively longer duration of immobilization and consequently decrease in the hand grip strength.
GCT of the distal radius is best treated with excision of the distal radius and reconstruction by non-vascularized fibula with good functional results[12].Our method of resection and reconstruction with non-vascularized fibular graft, internal fixation with DCP with primary bone grafting, use of stabilizing K-wires across the newly formed wrist joint and ligament reconstruction has been advocated by many other authors[13,14,15].
Clinical Message
ORIF with resection of distal end of radius and reconstruction with ipsilateral non-vascularised proximal fibula along with plate and 2 k-wires is a novel method for treating giant cell tumors of distal end of radius with all good results, excellent grip strength and with minimal complications. It also preserves the functional movement and stability with normal appearance of the wrist. Further, this procedure eliminates the need for microvascular surgery. Moreover, the anterior approach used in our study offers excellent and safe exposure of the radius.
Editor’s Note
The surgical treatment of a giant cell tumor located in the distal radius is dictated mainly by the Campanacci grading. It is accepted that the distal radius is one site where giant cell tumors have a very high rate of local recurrence. It is mainly because of the anatomical constraints and difficulty in achieving a complete intra lesional clearance. However, whenever possible, salvaging the wrist by intra lesional curettage and reconstruction has always shown much better functional outcomes as compared by the M.S.T.S. scoring system. This is possible when the disease is not involving the radio-carpal joint, the soft tissue extension is in only one plain and the residual bone stock is adequate. Campanacci grade 1 and 2 lesions and some grade 3 lesions may still be amenable to intra lesional curettage, though with a higher risk of local recurrence. This is compensated by the much better functional outcomes as compared with en bloc resections. The success of fibular reconstruction modality with wrist salvage would largely depend on regaining the wrist ligamentous and capsular stability, failure of which will result in stiff, painful wrist and carpal subluxation. Such a reconstructive modality may not be the preferred choice in very large Campanacci grade 3 lesions, wherein wrist arthrodesis either by bone graft or ulnar translocation technique gives excellent functional outcome with minimum risk of local recurrence.
References
1. Szendroi M. Giant cell tumor of bone. J Bone Joint Surg Br 2004;86:5-12.
2. Eckardt JJ, Grogan TJ. Giant cell tumour of bone. Clin Orthop. 1986;204:45–58.
3. Dahlin DC, Cupps RE, Johnson EW., Jr Giant cell tumour: A study of 195 cases. Cancer. 1970;25:1061–70.
4. Goldenberg RR, Campbell CJ, Bonfiglio M. Giant cell tumour of bone. An analysis two hundred and eighty cases. J Bone Joint Surg Am. 1970;52:619–64.
5. Campanacci M. Giant cell tumor and chondrosarcoma: grading, treatment and results. Cancer Res 1976;54:257-61.
6. Smith RJ, Mankin HJ. Allograft replacement of distal radius for giant cell tumor. J Hand Surg Am 1977;2:299-308.
7. Starr DE. Congenital absence of radius; method of surgical correction. J Bone Joint Surg 1945;27:572.
8. Parrish FF. Treatment of bone tumors by total excision and replacement with massive autologous and homologous grafts. J Bone Joint Surg Am 1966;48:968-90.
9. Murray JA, Schlafly B. Giant cell tumors in the distal end of the radius. Treatment by resection and fi bular autograft interpositional arthroplasties. J Bone Joint Surg Am 1986;68:687-94.
10. Pho RW. Malignant giant cell tumour of distal end of the radius treated by a free vascularized fibular transplant.J Bone Joint Surg Am. 1981;63:877–84.
11. Ihara K, Doi K, Sakai K, Yamamoto M, Kanchiku T, Kawai S. Vascularized fibular graft after excision of giant cell tumour of the distal radius.a case report. J Surg Oncol. 1998;68:100–3.
12. Goni V, Gill SS, Dhillon MS, Nagi ON. Reconstruction of massive skeletal defects after tumour resection. Ind J Orthop. 1992;26:13–6.
13. Deb HK, Das NK. Resection and reconstructive surgery in giant cell tumour of bone. Ind J Orthop.1992;26:13–6.
14. Dhamni IK, Jain AK, Maheswari AV, Singh MP. Giant cell tumours of the lower end of radius:problems and solutions. Ind J Orthop. 2005;39:201–5.
15. Saraf SK, Goel SC. Complications of resection and reconstruction in giant cell tumour of distal end of radius- An analysis. Ind J Orthop. 2005;39:206–11..
| How to Cite this article: Godghate N, Kadu VV, Saindane KA, Godghate NN. Non-Vascularised Ipsilateral Fibular strut – A Modality to Treat Giant cell tumor of lower end radius using Anterior Approach. Journal of Bone and Soft Tissue Tumors May-Aug 2015; 1(1):45-47. |

Dr. Ninad Godghate
|

Dr. Vikram V. Kadu
|

Dr. K. A. Saindane
|

Dr. Neha N Godghate
|
(Abstract) (Full Text HTML) (Download PDF)