Journal of Bone and Soft Tissue Tumors (JBST) License
![]()
Journal of Bone and Soft Tissue Tumors (JBST) by http://jbstjournal.com/ is licensed under https://creativecommons.org/licenses/by-nc-sa/4.0/
Based on a work at http://jbstjournal.com/.
Permissions beyond the scope of this license may be available at editor.jbst@gmail.com
Journal of Bone and Soft Tissue Tumors (JBST) is the official Journal of The Indian Musculo Skeletal Oncology Society

Denosumab Therapy Related Changes in Giant cell Tumor (Osteoclastoma) of Bone : A New Osteosarcoma Mimicker
Vol 4 | Issue 2 | July-Dec 2018 | Page 4-6 | Pradnya Manglekar, Sujit Joshi, Yogesh Panchwagh.
Authors: Pradnya Manglekar [1], Sujit Joshi [1], Yogesh Panchwagh [1].
[1] Dept. of Pathology Deenanath Mangeshkar Hospital and Research Centre, Pune
[2] Orthopaedic Oncology Clinic, Pune, India.
Address of Correspondence
Dr. Sujit Joshi,
Dept. of Pathology Deenanath Mangeshkar Hospital and Research Centre, Pune
Email: sujitjoshi30@gmail.com
Abstract
Objectives: Giant cell tumor (Osteoclastoma)of bone is locally aggressive osteolytic tumor. Denosumab–A monoclonal antibody against RANKL is recently being used to treat this tumor. We discuss histopathological changes occurring in giant cell tumor of bone after Denosumab treatment.
Method: A retrospective study of 12 cases from January 2014 to March 2018. All patients included were diagnosed as giant cell tumor (osteoclastoma) of bone on needle or open biopsy. Subsequently these patients received Denosumab therapy followed by surgical resection (extended curettage or wide excision). Histomorphological features after Denosumab therapy were evaluated in these specimens and compared with morphological features of prior biopsy samples.
Results: Needle or open biopsy samples studied prior to receiving Denosumab therapy showed typical morphological features of osteoclastoma i.e. presence of uniformly distributed osteoclastic cells and sheets of mononuclear stromal cells. No atypical mitoses or matrix production noted. Post Denosumab therapy resection specimens showed marked reduction in number of osteoclastic giant cells. There was predominance of mononuclear stromal cells along with abundant, irregular new bone (osteoid) formation with osteoid matrix deposition. Occasional mitotic activity was seen. Few foci of necrosis were noted.
Conclusion: Denosumab treatment causes significant giant cell depletion accompanied by abundant new bone formation separated by cellular stromal proliferation. These features bear very little resemblance to their pre-treatment counterparts and can mimic morphological features of osteosarcoma and other bone forming tumors. Hence, one should be aware of these changes so that a misdiagnosis of osteosarcoma can be avoided.
Keywords: Giant cell tumor (osteoclastoma), Denosumab, RANKL.
References
1. Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease.9th edition. Saunders Elsevier: Philadelphia; 2015. Chapter 26, Bones, Joints and Soft tissue tumors; p1179 – 1226.
2. Rosai J. Rosai and Ackerman’s Surgical Pathology. 10thedition. Elsevier Mosby: St.Louis, Missouri; 2011. Chapter 24, Bone and joints; p2013-2104.
3. Branstetter DG, Nelson SD, Manivel JC, Blay JY et al. Denosumab induces Tumor Reduction and Bone formation in Patients with Giant-Cell Tumor of Bone. Clin Cancer Res; 18(16); 4415-24.2012 AACR.
4. Singh AS, Chawla NS, Chawla SP. Giant-cell tumor of bone: treatment options and role of denosumab. Biologics: Targets and Therapy 2015;9, 69-74.
5. Huang L, Teng XY, Cheng YY, Lee KM, Kumta SM. Expression of preosteoblast markers and Cbfa-1 and Osterix gene transcripts instromal tumour cells of giant cell tumour of bone. Bone 2004 Mar;34 (3):p393–401.
6. James IE, Dodds RA, Olivera DL, Nuttall ME, Gowen M. Human osteoclastoma-derived stromal cells: correlation of the ability to form mineralized nodules in vitro with formation of bone in vivo. J Bone Miner Res 1996 Oct;11 (10):1453–60.
7. Wojcik J, Rosenberg AE, Bredella MA, et al. Denosumab-treated giant cell tumor of bone exhibits morphologic overlap with malignant giant cell tumor of bone. Am J SurgPathol 2016 Jan; 40(1): 72-80.
8. Rekhi B, Verma V, Gulia A, et al. Clinicopathological features of a series of 27 cases of post-denosumab treated giant cell tumors ofbones: a single institutional experience at a tertiary cancer referralcentre, India. PatholOncol Res 2017 Jan; 23 (1): 157-64.
9. Chang-Che Wu, Pin-Pen Hsieh. Denosumab-Treated Giant Cell Tumor of the Bone Mimicking Low-Grade Central Osteosarcoma.Journal of Pathology and Translational Medicine 2018; 52: 133-135.

(Abstract Full Text HTML) (Download PDF)
Like this:
JBST- Special APMSTS 2018 Issue
Vol 4 | Issue 2 | July-Dec 2018 | page:1 | Dr. Yogesh Panchwagh, Dr. Ashish Gulia, Dr. Ashok Shyam.
Author: Yogesh Panchwagh [1], Ashish Gulia [2], Ashok Shyam [1,3].
[1] Orthopaedic Oncology Clinic, Pune, India.
[2] Orthopedic Oncology Services, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai.
[3] Indian Orthopaedic Research Group, Thane, India,
[4] Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India
Address of Correspondence
Dr. Yogesh Panchwagh.
Orthopaedic Oncology Clinic, 101, Vasant plot 29, Bharat Kunj Society -2, Erandwana, Pune – 38, India.
Email: drpanchwagh@gmail.com
JBST- Special APMSTS 2018 Issue
It gives us immense pleasure in presenting the special IMSOS (Indian Musculoskeletal Oncology Society) issue of Journal of bone and soft tissue tumors on the occasion of the 12th Asia Pacific Musculoskeletal Tumor Society meeting, Jaipur, India. It’s only the second time, the first being in 2002, that APMSTS conference is being held in India. It is being co-hosted by the IMSOS, a relatively new body comprising of mostly the young but enthusiastic clinicians and paramedical staff involved in sarcoma care in India. Under the able presidentship of Dr Ajay Puri, a veteran in the field, the 12th APMSTS is all set to give the delegates a memorable experience. It’s but natural that Dr Ajay Puri, President – APMSTS 2018 and IMSOS has penned the guest editorial for this issue.
JBST (Journal of bone and soft tissue tumors) is proud to be associated with IMSOS as its official journal. All the members of IMSOS have contributed wholeheartedly to this issue echoing the theme of APMSTS 2018: “Education – Collaboration – Innovation”. The issue comprises of original articles on the data from institutes located across India on varied topics ranging from demographics of sarcoma in eastern India to osteosarcoma of facial bones from South India to recent topics like post denosumab changes in the histopathology of Giant cell tumors from western India. Even the case reports, which are rare clinical presentations of pathologies like osseous hydatid cyst, chordoma, clear cell chondrosarcoma, sacral inclusion cyst, hold a high educational value.
We also take this opportunity to invite all delegates to submit to Journal of Bone and Soft tissue tumors, which is one of the few journals that publish bone tumor research. We have a great editorial board and an online submission and review system. JBST has completed four years now and we are committed to make JBST the best resource for publishing bone tumor research in the world. This can be only achieved by co-operation and collaboration from all of you
We are happy to present this issue at the 12th APMSTS at Jaipur. Hope you will enjoy it as much as the vibrant, colourful and warm Indian hospitality.
Dr. Yogesh Panchwagh
Dr. Ashish Gulia
Dr. Ashok Shyam
(Abstract Full Text HTML) (Download PDF)
Like this:
Need for a dedicated Musculoskeletal Tumor Registry in India
Vol 3 | Issue 1 | May- Aug 2017 | page:1 | Dr. Yogesh Panchwagh & Dr. Ashok Shyam.
Author: Dr. Yogesh Panchwagh [1], Dr. Ashok Shyam [2,3].
[1]Orthopaedic Oncology Clinic, Pune, India.
[2] Indian Orthopaedic Research Group, Thane, India
[3] Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India
Address of Correspondence
Dr. Yogesh Panchwagh.
Orthopaedic Oncology Clinic, 101, Vasanth plot 29, Bharat Kunj Society -2, Erandwana, Pune – 38, India.
Email: drpanchwagh@gmail.com
Need for a dedicated Musculoskeletal Tumor Registry in India
Registries are one of the most important resources for any disease. Around 200 cancer registries in the world that covering up mere 5% of worlds population was noted in 1999. However no parallel data exists currently but we are sure that number of cancer registries have increased over the period of time.India has an already existing National cancer registry program which was started in 1981 and is still running strong. However we belive that time has now come for a dedicated musculosketal registry in India. The technology has grown rapidly and now we have developed a simple mobile app which can collect most of the registry data in a very simple and user friendly way. We have been working on this concept sicne two years now and have taken inputs from many orthoonco surgeons. The mobile app is finally launched in the public domain and is available on google play store and app store. The app is named ‘MSK Registry’ and It can be downloaded for free by all interested in contributing cases. We would urge everyone to contribute and also write to us for any issues or queries
Regards.
Dr Yogesh Pachwagh
Dr Ashok Shyam
Yogesh Panchwagh & Ashok Shyam
Registry in India. Journal of Bone and Soft Tissue Tumors Sep-Oct 2017; 3(1):1.
(Abstract Full Text HTML) (Download PDF)
Like this:
Plantar Fibromatosis Masquerading as Liposarcoma : a Case Report and Review of Literature
Volume 2 | Issue 2 | May-Aug 2016 | Page 25-29 | Nishit Bhatnagar, Purushotham Lingaiah, Sumit Arora, Anil Dhal.
Authors: Nishit Bhatnagar [1], Purushotham Lingaiah [1], Sumit Arora [1], Anil Dhal [1].
[1]Department of Orthopaedic Surgery, Maulana Azad Medical College & associated Lok Nayak Hospital, New Delhi-110002
Address of Correspondence
Dr. Nishit Bhatnagar
7 Godavari Apartments, Alaknanda, New Delhi – 19
E-mail id: nishitbhatnagar@yahoo.co.in
Abstract
Plantar fibromatosis and well differentiated liposarcoma can have a similar clinical presentation of a slow growing superficial well defined mass on the plantar aspect of foot. We present a patient of plantar fibromatosis mimicking a lipomatous tumour of the foot. Marginal resection of the remaining tumour was performed. At two years postoperatively, there has been no recurrence of the tumour.
Keywords: liposarcoma, foot, plantar fibromatosis
Introduction
Plantar fibromatosis is a benign lesion involving the plantar aponeurosis. Ledderhose [1] in 1897 reported and described approximately 50 cases of contractures of the plantar fascia, leading to the entity being termed as Ledderhose’s disease. Its similarity to Dupuytrens’s disease of the hand has also led to the term “Dupuytren’s disease of the plantar fascia” [2]. It is commonly known to occur in the 3rd to 5th decade of life, has a male preponderance and is bilateral in 20 to 50% of cases [3,4,5]. It has an unknown etiology and is characterized by neoplastic proliferation of immature fibroblasts with spindle-shaped myofibroblasts within the plantar fascia [6]. They can be locally aggressive, demonstrate local recurrence but do not metastasize. Lipogenic tumours represent the most common soft tissue tumours [7]. Atypical and malignant lipomatous neoplasms are the most common variety of adult soft tissue sarcomas, accounting for nearly 20% of all sarcomas [8]. Lipomatous tumours are most frequently found in the extremities, retroperitoneum, groin and abdominal wall [9]. Lipomatous tumours can range from benign lipomas to highly malignant dedifferentiated liposarcomas [10]. Nomenclature and classification of lipomatous tumours has undergone major changes over time. Based on cytogenetic and molecular genetic studies, liposarcomas were classified by the World Health Organization Committee for classification of soft tissue tumours into five subtypes, atypical/well-differentiated liposarcoma, dedifferentiated liposarcoma, myxoid liposarcoma (including high grade round cell liposarcoma), pleomorphic liposarcoma and a rare mixed-type liposarcoma [8]. Some workers have proposed that the term ‘atypical lipomatous tumour’ should be used for tumours arising from extremities and chest wall, whereas ‘well differentiated liposarcoma’ should be used for describing tumours arising in the retroperitoneum and abdominal cavity [11,12,13]. Diagnosis of well differentiated liposarcomas of the extremities can be delayed due to relatively benign symptomatology and a low index of suspicion. Plantar fibromatosis and well differentiated liposarcoma can have a similar clinical presentation of a slow growing superficial well defined mass on the plantar aspect of foot. Here we present a patient of plantar fibromatosis mimicking a lipomatous tumour of the foot.
Case presentation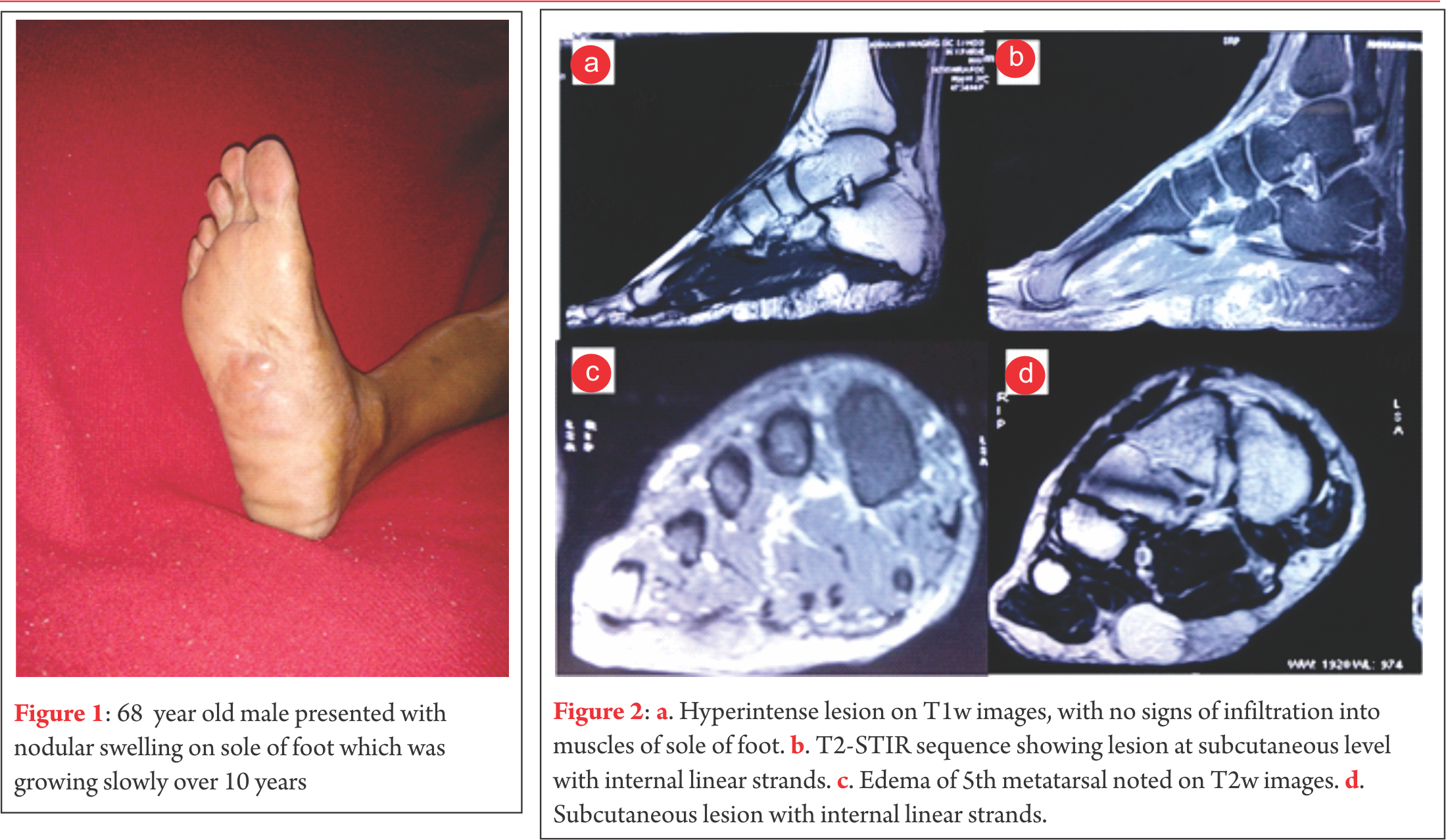 A diagnosis of plantar fibromatosis was made, keeping lipoma as a differential diagnosis. Plain radiographs showed no bony pathology. An unsuccessful trial of oral analgesics and customized insole was given. Prior to operative intervention for the mass on the plantar aspect of foot an excisional biopsy of the mass on the lateral border of the foot was performed. The biopsy revealed nodular non-encapsulated fibrofatty tissue on gross examination. Histopathological examination revealed nodular proliferation of adipocytes and myofibroblasts separated by collagenous bands. The nodules of fatty tissue showed a mixture of mature and immature fat cells with multivacuolation and nuclear indentation. Nuclear pleomorphism, hyperchromasia and mitosis were observed leading to a diagnosis of well differentiated liposarcoma. MRI revealed a 6.5cm x 6.6cm x 2cm well circumscribed, multilobulated lesion along the plantar aspect of the mid foot at the subcutaneous level that appeared to be indistinguishable from surrounding subcutaneous fat with internal linear strands. It was seen to insinuate between medial and lateral heads of plantar aponeurosis, however it did not show infiltration into the muscles of sole of the foot. Overlying skin of sole of foot appeared uninvolved. The lesion was hyperintense on T1w images, however suppresses completely on T2-STIR sequences. Few linear strands are noted tha are isointense in T1w images and showed enhancement in post contrast images (Fig. 2). Except for subtle focal edema in the base of the fifth metatarsal there was no bony involvement. Marginal resection of the remaining tumour was performed through an S-shaped incision on the non-weight bearing area of the sole. Tumour tissue was found to be lying between the dermis and the plantar aponeurosis. It was observed to be comprised of friable adipose tissue with a few intervening fibrotic septae. Tumor was non-encapsulated, however it could be easily separated from rest of the neighbouring structures. The adjacent aponeurosis and dermis appeared to be free of any gross tumour infiltration. The medial plantar neurovascular bundle also appeared free from any tumour infiltration. Histology revealed nodules of mature and immature adipose tissue separated by fibrovascular septae with areas of increased cellularity, pleomorphism, hyperchromasia and tumour giant cells (Fig. 3).
A diagnosis of plantar fibromatosis was made, keeping lipoma as a differential diagnosis. Plain radiographs showed no bony pathology. An unsuccessful trial of oral analgesics and customized insole was given. Prior to operative intervention for the mass on the plantar aspect of foot an excisional biopsy of the mass on the lateral border of the foot was performed. The biopsy revealed nodular non-encapsulated fibrofatty tissue on gross examination. Histopathological examination revealed nodular proliferation of adipocytes and myofibroblasts separated by collagenous bands. The nodules of fatty tissue showed a mixture of mature and immature fat cells with multivacuolation and nuclear indentation. Nuclear pleomorphism, hyperchromasia and mitosis were observed leading to a diagnosis of well differentiated liposarcoma. MRI revealed a 6.5cm x 6.6cm x 2cm well circumscribed, multilobulated lesion along the plantar aspect of the mid foot at the subcutaneous level that appeared to be indistinguishable from surrounding subcutaneous fat with internal linear strands. It was seen to insinuate between medial and lateral heads of plantar aponeurosis, however it did not show infiltration into the muscles of sole of the foot. Overlying skin of sole of foot appeared uninvolved. The lesion was hyperintense on T1w images, however suppresses completely on T2-STIR sequences. Few linear strands are noted tha are isointense in T1w images and showed enhancement in post contrast images (Fig. 2). Except for subtle focal edema in the base of the fifth metatarsal there was no bony involvement. Marginal resection of the remaining tumour was performed through an S-shaped incision on the non-weight bearing area of the sole. Tumour tissue was found to be lying between the dermis and the plantar aponeurosis. It was observed to be comprised of friable adipose tissue with a few intervening fibrotic septae. Tumor was non-encapsulated, however it could be easily separated from rest of the neighbouring structures. The adjacent aponeurosis and dermis appeared to be free of any gross tumour infiltration. The medial plantar neurovascular bundle also appeared free from any tumour infiltration. Histology revealed nodules of mature and immature adipose tissue separated by fibrovascular septae with areas of increased cellularity, pleomorphism, hyperchromasia and tumour giant cells (Fig. 3). 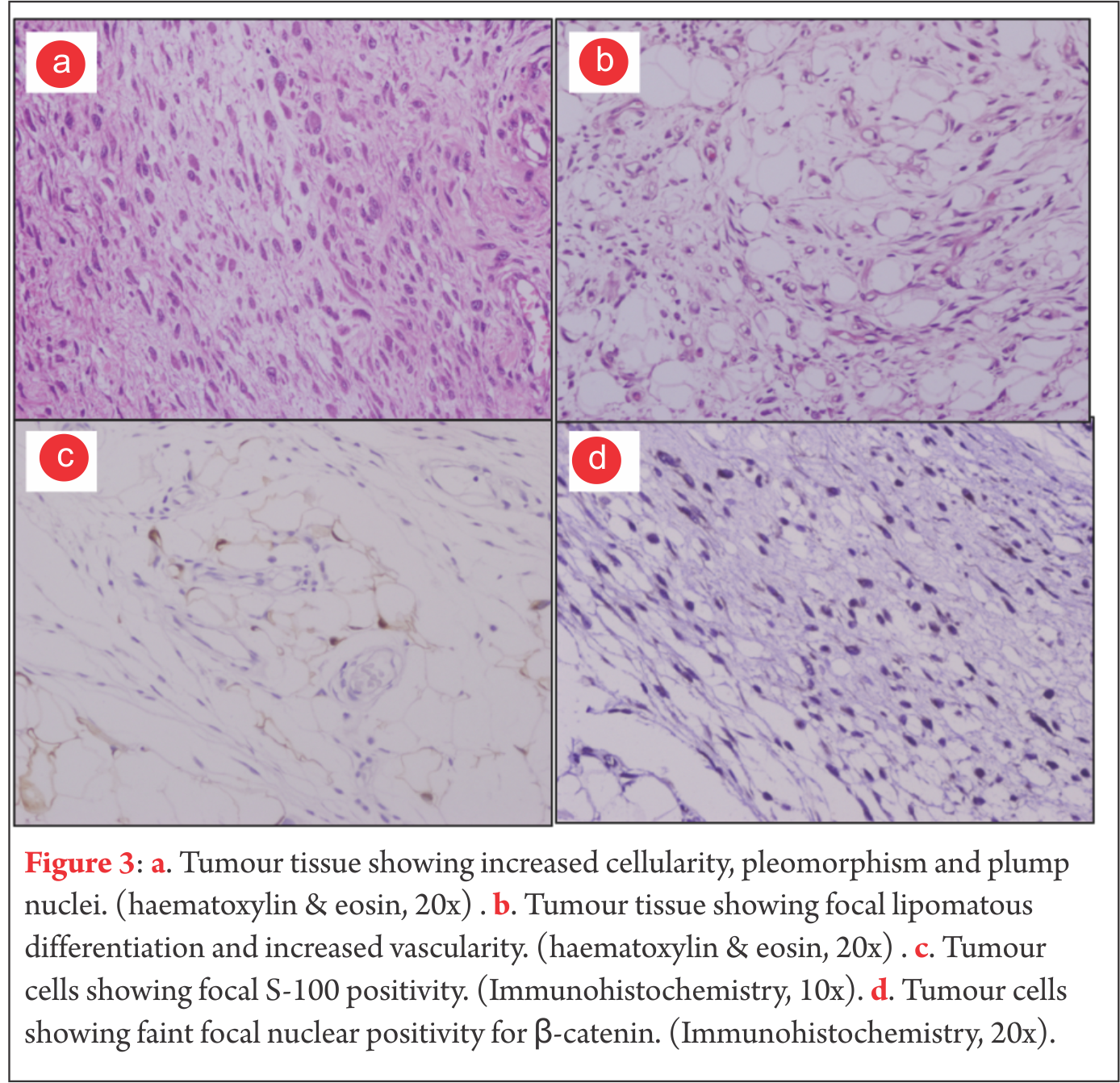 Mitotic figures were rare. Occasional cell with lipoblast like morphology was seen. Focal S-100 positivity was seen. Fatty tissue adherent to the skin also showed lesion cells in them. Due to proximity of tumour to the skin of the sole, thin skin flaps had to be created. Postoperatively marginal skin necrosis was observed and wound healing was delayed. Patient did not receive any postoperative chemotherapy or radiotherapy. At two years postoperatively, there has been no recurrence of the tumour and patient is able to ambulate without any discomfort. Patients consent was solicited before publishing the report
Mitotic figures were rare. Occasional cell with lipoblast like morphology was seen. Focal S-100 positivity was seen. Fatty tissue adherent to the skin also showed lesion cells in them. Due to proximity of tumour to the skin of the sole, thin skin flaps had to be created. Postoperatively marginal skin necrosis was observed and wound healing was delayed. Patient did not receive any postoperative chemotherapy or radiotherapy. At two years postoperatively, there has been no recurrence of the tumour and patient is able to ambulate without any discomfort. Patients consent was solicited before publishing the report
A 68-years-old male of Indian subcontinent was referred to our department with a ten year history of slow growing nodular masses on the non-weight bearing part of sole and along the lateral border of the right foot. The mass on the sole of the foot had become painful over the last one year. The masses were superficial, well defined, mildly tender and soft to firm in consistency (Fig. 1).
Discussion
Liposarcomas of the extremities are the second most commonly encountered soft tissue sarcoma after fibrous / fibrohistiocytic malignancies [14]. They occur almost exclusively in the age group between 40 to 60 years of age [14,15]. Liposarcomas are commonly encountered in the lower extremity, usually in the thigh, but rarely in the foot. Enzinger et al analyzed 1067 cases of liposarcoma, but none of them were in the foot [16]. There have been very few cases of liposarcomas of the foot reported in literature [17,18,19,20]. Preoperative diagnosis is infrequent. Hence, increasing the understanding of this tumour is important. WHO has categorized liposarcoma into five subtypes, out of which the well-differentiated variety is the most common, accounting for approximately 40% to 50% of all liposarcomas [21,14,22]. According to Evans et al a ‘well-differentiated liposarcoma’ and ‘atypical lipoma’ are identical in biological, behaviour, histological and karyotypic characteristics [23]. The term well differentiated liposarcoma is better used for lipomatous lesion in regions where wide resection is not possible (mediastinum and retroperitoneum), whereas the tumour is considered to be an atypical lipoma in other locations. Clinically, liposarcomas usually present as a painless soft tissue mass. Only around 10-15% liposarcomas present as a painful soft tissue mass [14]. These can be easily confused with fibromatosis which presents as slow growing single or multiple painful nodular thickenings [24]. A lipoma and a well-differentiated liposarcoma are also quite similar in clinical presentation. MR imaging is an essential tool for detection of liposarcoma as well as for studying its locoregional extension and relations (bone, soft-tissues and neurovascular involvement). MRI can help in differentiating between lipoma, liposarcoma and fibromatosis. Well-differentiated liposarcomas typically demonstrate a largely lipomatous mass, hyperintense on TW1 images, representing over 75% of the lesion in a nodular arrangement separated by thick non-lipomatous septae (>2mm but not exceeding 2cm). The non-lipomatous component shows variable enhancement on fat saturated T1w contrast enhanced images [25,26]. Lipomas also demonstrate abundant adipose tissue homogenously hyperintense on T1w images, similar to well-differentiated liposarcomas. However, lipomas have thin septae (<2mm) and contrast enhancement of lower signal intensity [21]. Fibromatosis on MRI shows nearly the same low-signal intensity as adjacent muscle on T1w and T2w images. Majority of fibromatosis show marked enhancement on gadolinium administration [27,28]. MRI must be performed prior to biopsy or any therapeutic management of a suspected liposarcoma. A well-differentiated liposarcoma appears grossly like a well-circumscribed multi-lobulated mass. Some sections of the tumour reveal mature adipose tissue in abundance that appears identical to a lipoma. However, a well-differentiated liposarcoma can be histologically identified by a typical scattering of lipoblasts with irregularly shaped hyperchromatic nuclei, along with thick fibrovascular septae [16]. Immunohistochemical analysis helps to distinguish a lipoma from a well-differentiated liposarcoma. MDM2 and CDK4 markers are expressed by a well-differentiated liposarcoma [29]. Fibromatosis can be identified based on its characteristic nodular cellular proliferation of plump, spindle shaped cells with intervening collagen with infrequent mitotic figures [30]. Well-differentiated liposarcomas are not known to have malignant potential but local recurrence risk is high [31]. For such tumours of the extremity, the local recurrence rate can be as high as 43% [32]. Such tumours are also reported to have undergone dedifferentiation into a more aggressive form with higher risk of local recurrence and metastasis [9].Prognosis and management of these tumours is related to their anatomical location. Most authors suggest that subcutaneously located tumours can be treated by wide resection, with minimal chances of local recurrence. Radiotherapy is not recommended unless there is gross residual tumour tissue. Chances of recurrence are much higher for tumours in deeper locations. Local recurrence can be treated by re-excision and radiotherapy [32,33,34]. Asymptomatic or mildly symptomatic lipomas of the extremity can be managed conservatively. Troublesome lipomas can be treated by simple excision. The management of fibromatosis can range from conservative management, intralesional steroid injections, collagenase injections, radiotherapy to surgical excision [35,36,37,38,39]. Due to such different lines of management of these pathologies, it is imperative to establish the correct diagnosis before proceeding to treatment. In this case, clinical presentation suggested a diagnosis of plantar fibromatosis, imaging studies suggested the possibility of a lipomatous tumour and histopathological evidence rasied the suspicion of a well differentiated liposarcoma. However, the final diagnosis of plantar fibromatosis was established after correlating the clinical features with a definitve histopathological evaluation following excision of the mass.
conclusions
Although plantar fibromatosis is a commonly encountered disease, it can be mimicked by rare pathologies like lipoma and liposarcoma. Hence, a high index of suspicion is required for their early diagnosis and proper surgical management. Management decisions should be taken after careful correlation between clinical, radiological and histopathological features.
References
1. Ledderhose H. Zur Pathologie der Aponeurose des Fusses und der Hand. Langenbecks Arch Klin Chir. 1897;55:694-712.
2. Cavolo DJ, Sherwood GF. Dupuytrens’s disease of the plantar fascia. J Foot Surg. 1982.21(1):12-15.
3. Weiss SW, Goldblum JR, Enzinger FM. Fibromatoses. In: Weiss SW, Goldblum JR editors. Enzinger and Weiss’ Soft Tissue Tumors. Philadelphia, Pa, USA: Mosby Elsevier;2008. p. 227–228.
4. Lee TH, Wapner KL, Hecht PJ. Plantar fibromatosis. J Bone Joint Surg Am. 1993;75(7):1080–1084.
5. Aviles E, Arlen M, Miller T. Plantar fibromatosis. Surgery. 1971;69(1):117–120.
6. Zgonis T, Jolly GP, Polyzois V, Kanuck DM, Stamatis ED. Plantar fibromatosis. Clin Podiatr Med Surg. 2005;22(1):11-18.
7. Mentzel T, Fletcher CD: Lipomatous tumours of soft tissues: An update. Virchow’s Arch. 1995; 427(4): 353-363.
8. Fletcher CDM, Unni KK, Mertens F. World Health Organization Classification of Tumours. In: Fletcher CDM, Unni KK, Mertens F, editors. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon:IARC Press; 2002. p. 9-18.
9. Weiss SW, Rao VK. Welldifferentiated liposarcoma (atypical lipoma) of deep soft tissue of the extremities, retroperitoneum, and miscellaneous sites. A follow-up study of 92 cases with analysis of the incidence of “Dedifferentiation”. Am J Surg Pathol 1992;16(11):1051-1058.
10. Dei Tos AP. Liposarcoma: New entities and evolving concepts. Ann Diagn Pathol. 2000;4(4):252-266.
11. Fletcher CD. Soft tissue tumours. In: Fletcher CD, editor. Diagnostic histopathology of tumours. 2nd edition. London:Harcourt Publishers Limited; 2000:1473–1540.
12. Kindblom LG, Angervall L, Fassina AS. Atypical lipoma. Acta Pathol Microbiol Immunol Scand [A]. 1982;90(1):27–36.
13. Evans HL, Soule EH, Winkelmann RK. Atypical lipoma, atypical intramuscular lipoma, and well differentiated retroperitoneal liposarcoma: a reappraisal of 30 cases formerly classified as well differentiated liposarcoma. Cancer. 1979;43(2):574–584.
14. Peterson JJ, Kransdorf MJ, Bancroft LW, O’Connor MI. Malignant fatty tumours: classification, clinical course, imaging appearance and treatment. Skeletal Radiol. 2003;32(9):493-503.
15. Munk PL, Lee MJ, Janzen DL, Connell DG, Logan PM, Poon PY, Bainbridge TC. Lipoma and liposarcoma: evaluation using CT and MR imaging. AJR Am J Roentgenol. 1997;169(2):589-594.
16. Enzinger FM, Weiss SW. Liposarcoma. In: Weiss SW, Goldblum JR, Folpe AL, editors. Soft Tissue Tumors. 3rd edition. St. Louis, Mosby, USA: Mosby Elsevier;1995:686-697.
17. Sugar S, Murphy BM. Liposarcoma of the foot; case report. J Mich State Med Soc. 1955;54(4):468–469.
18. Kelly PC, Shramowiat M. Liposarcoma of the foot: a case report. J Foot Surg. 1978;17(1):27–31.
19. Rajasekhar C, Paul AS, Bale RS. Spindle-cell liposarcoma: a rare variant of liposarcoma arising in the foot. Clin Oncol (R Coll Radiol). 2005;17(2):128–129.
20. Matsuo T, Sugita T, Shimose S, Kubo T, Yasunaga Y, Ochi M. Liposarcoma arising in the foot: a case report. Case Rep Med. 2009;2009:630203.
21. Kansdorf MJ, Bancroft LW, Peterson JJ, Murphey MD, Foster WC, Temple HT. Imaging of fatty tumours: distinction of lipoma and well-differentiated liposarcoma. Radiology. 2002;224(1):99-104.
22. Murphey MD, Arcara LK, Fanburg-Smith J. Imaging of musculosketal liposarcoma with radiologic-pathologic correlation. Radiographics 2005;25(5):13711395.
23. Evans H. Liposarcoma: a study of 55 cases with a reassessment of its classification. Am J Surg Pathol. 1979;3(6):507-523.
24. Chokshi FH, Jose J, Clifford PD. Plantar fibromatosis. Am J Orthop. 2009;38(9):475-476.
25. Matsumoto K, Takada M, Okabe H, Ishizawa M. Foci of signal intensities different from fat in well-differentiated liposarcoma and lipoma: correlation between MR and histological findings. J Clin Imaging. 2000;24(1):38-43.
26. Galant J, Martí-Bonmatí L, Sáez F, Soler R, Alcalá-Santaella R, Navarro M. The value of fat-suppressed T2 or STIR sequences in distinguishing lipoma from well-differentiated liposarcoma. Eur Radiol. 2003;13(2):337-343.
27. Walker EA, Petscavage JM, Brian PL, Logle CI, Montini KM, Murphey MD. Imaging features of superficial and deep fibromatoses in the adult population. Sarcoma [Internet]. 2012;2012. Epub 2012 Jun 28, Article ID 215810, 17 pages. Available from Hindawi at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3395298/pdf/SRCM2012-215810.pdf
28. Morrison WB, Schweitzer ME, Wapner KL, Lackman RD. Plantar fibromatosis: a benign aggressive neoplasm with a characteristic appearance on MR images.Radiology. 1994;193(3):841-845.
29. Shimada S, Ishizawa T, Ishizawa K, Matsumura T, Hasegawa T, Hirose T. The value of MDM2 and CDK4 amplification levels using real time polymerase chain reaction for the differential diagnosis of liposarcomas and their histologic mimickers. Hum Pathol. 2006;37(9):1123-1129.
30. Fetsch JF, Laskin WB, Miettinen M. Palmar-plantar fibromatosis in children and preadolescents: a clinicopathologic study of 56 cases with newly recognized demographics and extended follow-up information. Am J Surg Pathol. 2005;29(8):1095-1105.
31. Forus A, Larramendy ML, Meza-Zepeda LA, Bjerkehagen B, Godager LH, Dahlberg AB, Saeter G, Knuutila S, Myklebost O. Dedifferentiation of a welldifferentiated liposarcoma to a highly malignant metastatic osteosarcoma:amplification of 12q14 at all stages and gain of 1q22-q24 associated with metastases. Cancer Genet Cytogenet. 2001;125(2):100-111.
32. Kindblom LG, Angervall L, Svendsen P. Liposarcoma a clinicopathologic, radiographic and prognostic study. Acta Pathol Microbiol Scand Suppl. 1975;(253):1-71.
33. Kang J, Botros M, Goldberg S, Giraud C, Nielsen GP, Chen YL, Raskin K, Schwab J, Yoon SS, Hornicek FJ, Delaney TF. The Use of Radiation Therapy in the Management of Selected Patients with Atypical Lipomas. Sarcoma [Internet]. 2013;2013. Epub on 2013 Jan 15, Article ID 485483, 5 pages. Available from Hindawi at: http://www.hindawi.com/journals/sarcoma/2013/485483/
34. Sommerville SM, Patton JT, Luscombe JC, Mangham DC, Grimer RJ. Clinical outcomes of deep atypical lipomas (well-differentiated lipoma-like liposarcomas) of the extremities. ANZ Journal of Surgery. 2005;75(9):803–806.
35. Sammarco GJ, Mangone PG. Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21(7):563-569.
36. Hammoudeh ZS. Collagenase Clostridium histolyticum injection for plantar fibromatosis (Ledderhose disease). Plast Reconstr Surg. 2014;134(3):497e-498e.
37. Grenfell S, Borg M. Radiotherapy in fascial fibromatosis: a case series, literature review and considerations for treatment of early-stage disease. J Med Imaging Radiat Oncol. 2014;58(5):641-647.
38. McNally EG, Shetty S. Plantar fascia: imaging diagnosis and guided treatment. Semin Musculoskelet Radiol. 2010;14(3):334-343.
39. Aluisio FV, Mair SD, Hall RL. Plantar fibromatosis: treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int. 1996;17(11):672-678.
(Abstract Full Text HTML) (Download PDF)
Like this:
Rehabilitation following Limb-Salvage Surgery in Sarcoma
Volume 2 | Issue 2 | May-Aug 2016 | Page 20-24 | Vincent S Paramanandam, Anuradha A Daptardar, Ashish Gulia
Authors: Vincent S Paramanandam [1], Anuradha A Daptardar [1], Ashish Gulia [2].
1Physiotherapy Department, Tata Memorial Hospital, Mumbai
2Orthopedic Oncology Services, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai.
Address of Correspondence
Dr. Paramanandam V
Technichal Officer C, Physiotherapy Department, Tata Memorial Hospital, Mumbai
Email: vinsu24@gmail.com
Abstract
Introduction: Limb salvage after tumor resection has become a norm in today’s era. There are number of biological and non biological reconstruction options available for the reconstruction of these bone defects. The success story of these surgical procedures is mainly based on their excellent functional outcome. Post surgical rehabilitation plays an important role in achieving optimal functional outcome and good quality of life. The rehabilitation protocol following limb salvage surgery is complex and it differs with type of reconstruction procedure. Present articles discusses in detail the various rehabilitation protocols required to achieve above goals.
Keywords: Limb salvage surgery, rehabilitation, sarcoma
Introduction
Until 1970, amputation was the primary surgical treatment offered to bone and soft tissue sarcomas. However, from that time the treatment options have evolved dramatically and now approximately 90% of these cases undergo Limb Salvage Surgery (LSS)[1]. LSS has become the main line of treatment option for bone and soft tissue sarcomas along with adjuvant and/or neo adjuvant treatment modalities (Chemotherapy/ radiotherapy). The overall survival rate has been estimated as 55%-65%, based on the age of diagnosis, and it is considered to be comparable to that of amputation.
LSS is considered to be less invasive, provides better function and quality of life than amputation [2]. Moreover, it has been proposed that patients’ acceptability of LSS is high in view of the fact that it restores the body image better than amputation[3]. Nevertheless, LSS, unlike amputation, is associated with more peri-operative complications, prolonged hospital stay and requires repeated surgeries due to various reasons such as infection and prosthetic failure. LSS demands high surgical skills, whereas, amputation is a simple surgical procedure. Additionally, recent progress in prosthetic limbs, for example microprocessor based joints and endo-skeletal prosthetic reconstructions, have improved the functional outcome and cosmetic outlook following amputation [4]. A systematic review conducted by Bekkering et al [5] reported that the quality of life outcome from current available evidence is inconclusive in supporting LSS or amputation. Another recent systematic review and meta-analysis concluded that both surgical procedures provides similar functional recovery and quality of life [6].Despite the fact that early physical rehabilitation is the key to achieve good functional outcome and quality of life after LSS, rehabilitation techniques following LSS is largely neither tested nor documented in detail [7]. Lack of adequate early rehabilitation measures following LSS could be one of the rationales for conflicting interests reported by various studies examining the quality of life in LSS vs amputation.Hence, we have attempted to summarise basic principles and site specific considerations one must utilise to develop individual case specific rehabilitation protocol.
Common rehabilitation principles in LSS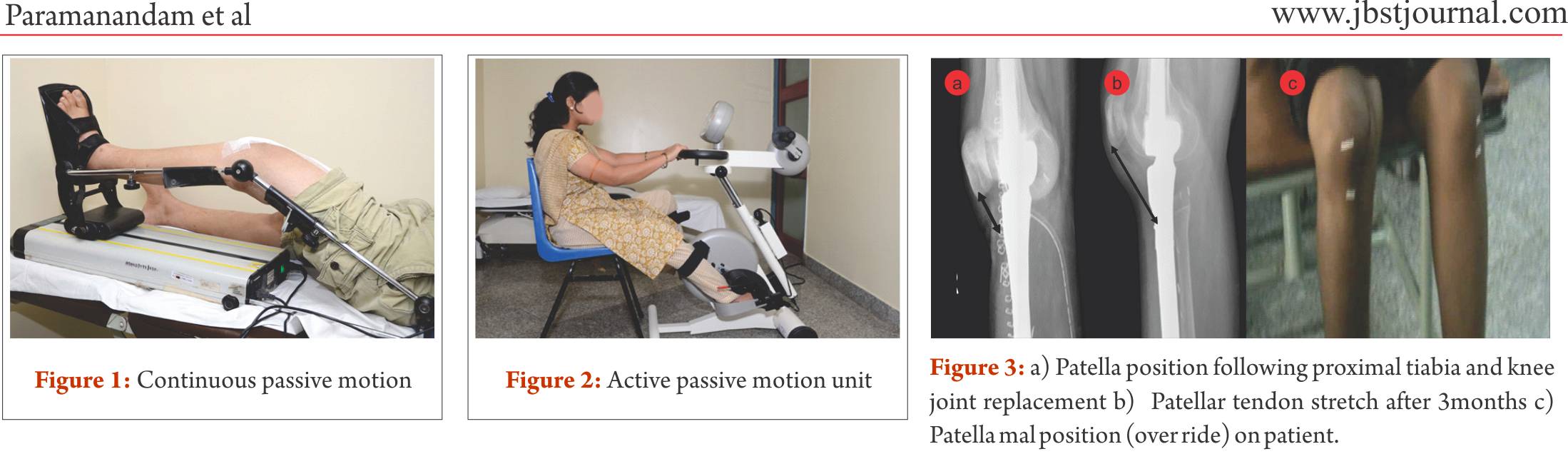
In a recent paper, Shehadeh et al. [7] attempted to standardize the rehabilitation protocol for LSS following high grade bone and soft tissue sarcomas. They reported that following a standardized rehabilitation protocol produced improved functional outcome in group of 59 patients with LSS. Their conclusion, however, is based on small observational study with heterogeneous population who received different type of LSS for different anatomical sites. Following set protocol in LSS, unlike general orthopaedic procedure, will be counterproductive. In general orthopaedic procedures, more or less,
specific anatomical structures are involved with minimal damage to the bone, joint and soft tissue structures. In contrast, in LSS following sarcomas, these structures are extensively resected and may not be identical between two individuals undergoing similar procedures for a particular site. For example, resection length for distal end of femur osteogenic sarcoma may depend on the extent of disease in two individuals [4]. Following are common rehabilitation prospectives that need to be considered to formulate comprehensive rehabilitation protocol for LSS.
Bone and joint reconstructions: Stability and mobility following LSS largely depends on the bone and joint structure loss and the type of reconstruction. For example, megaprosthetic distal femur replacement with cementing will allow the patient to be ambulated full weight bearing (FWB), whereas, if it is a bone graft , like in most of biological reconstructions, weight bearing needs to be delayed till the osteosynthesis is confirmed by radiographical evaluation.
Neuromuscular loss: Oncology resection demands large resections, which will also include a part of uninvolved soft tissue cover as surgical margin. Large resection may require additional rotational or free flaps for soft tissue coverage. In addition, nearby neuro-vascular bundle may need to be excised or repaired, hence, complete evaluation of neuro-motor loss would be necessary to plan the dynamic strength training and external support requirements.
Skin involvement: Donor sites of free flaps often receive split thickness skin graft which may hinder the early mobilisation of nearby joint. Moreover, scar development following open biopsy and LSS may need special attention from the rehabilitation team to prevent any future functional loss.
External supports: Temporary or permanent external support in the form of static or dynamic splinting may be required to provide support to the limb. To exemplify, prophylactic use of abduction brace along with derotation boot to prevent hip dislocation following proximal femur replacement and dynamic cock-up splint for radial nerve palsy needs to be the integral part of rehabilitation service.
Oncology treatments: Deranged blood count often hinders with the intensity of rehabilitation; hence, it prolongs the overall rehabilitation(8). Radiation induced fibrosis could cause severe restrictions in the joint range of motion. Thus, rehabilitation professionals must plan around the chemotherapy cycles and add prophylactic measures to prevent any impending radiation induced joint and soft tissue dysfunction.
Multidisciplinary approach: Limb salvage surgery is complex and demands close concordance in treatment specific outcomes between various health professional working in the rehabilitation team. This team may comprise of surgeons, medical oncologists, radiation therapists, nurses, physiotherapists, occupational therapists, prosthetics orthotics and medical social workers. Prehabilitation, rehabilitation even before starting the primary cancer therapy and surgery, such as crutch muscles strengthening, would be greatly beneficial in post-treatment functional outcome. Although in the field of LSS evidence of prehabilitation is lacking, there are considerable evidence to show beneficial effects in overall rehabilitation following cancer therapies [9–11].
Rehabilitation prescriptions and follow-up: Rehabilitation protocol for LSS must be tailor made considering the general principles and site specific modification, hence specific and also progressive. However, some negative effects of adjuvant therapies, such as the deranged blood counts and infection, may alter the course of rehabilitation process. Thus, frequent follow-up and close monitoring may be required during adjuvant therapy till they are functionally independent.
Rehabilitation consideration for specific sites
Site specific rehabilitation principles following LSS have been presented below for few common sites.
Mega prosthetic replacement for distal femoral resection:
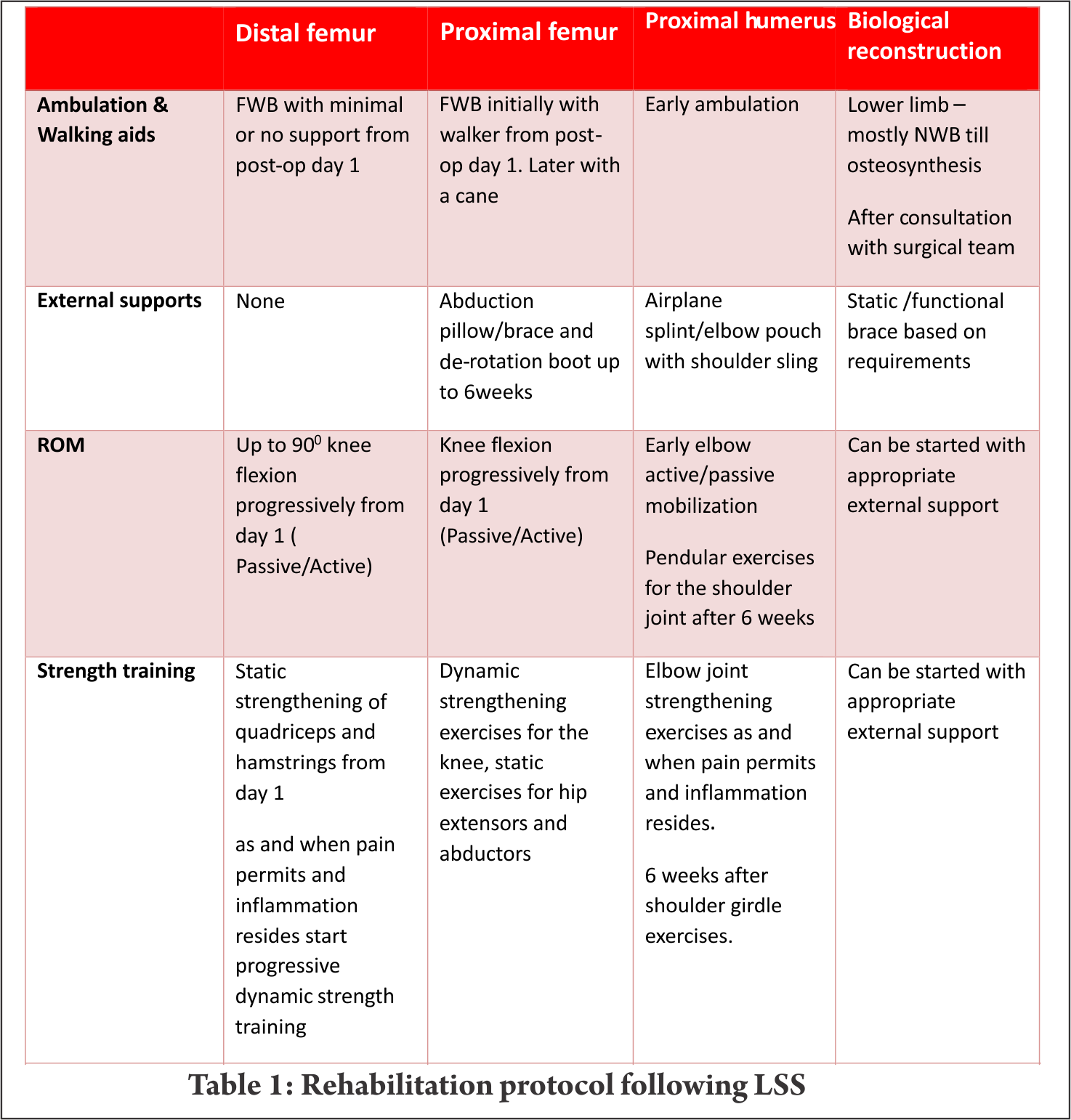
Distal femur is the commonest site for primary high grade sarcoma and giant cell tumors. Overall strengthening other than the affected site, in all possibility, should begin preoperatively. Limb elevation and ankle toe movement should be encouraged from post operative day one to prevent deep vein thrombosis. Cemented and semiconstrained (allows rotations and flexion/extension) knee joint endoprosthetic replacement permits early joint mobilization and FWB walking. Unlike other centres [4,7], in our centre knee joint mobilisation starts from day one with the help of continuous passive motion units (Fig.1) and active assisted methods within the pain tolerance level unless tight suturing. Close communication between the surgical team and the rehabilitation team helps in personalising the rehabilitation protocol as per the patients’ requirements. With adequate pain relief through appropriate medical management, active exercises could be started from day one to three. Full weight bearing walking could be started from day one initially with walker and later without any support if patient could effectively extend the knee “locking the knee”. Prior to ambulation, one leg standing and spot marching must be encouraged with appropriate support. After acute inflammation subsides slow progressive muscle strengthening exercises must be encouraged with the goal of achieving 900knee flexion, complete knee extension and muscle strength equivalent to the contra lateral lower limb by end of three months. Active passive motion devices, such as the one shown in Fig. 2, may help in joint mobilisation and strengthening. Summary of rehabilitation protocol is tabulated in Table 1.
Mega prosthetic replacement for proximal tibial resection:
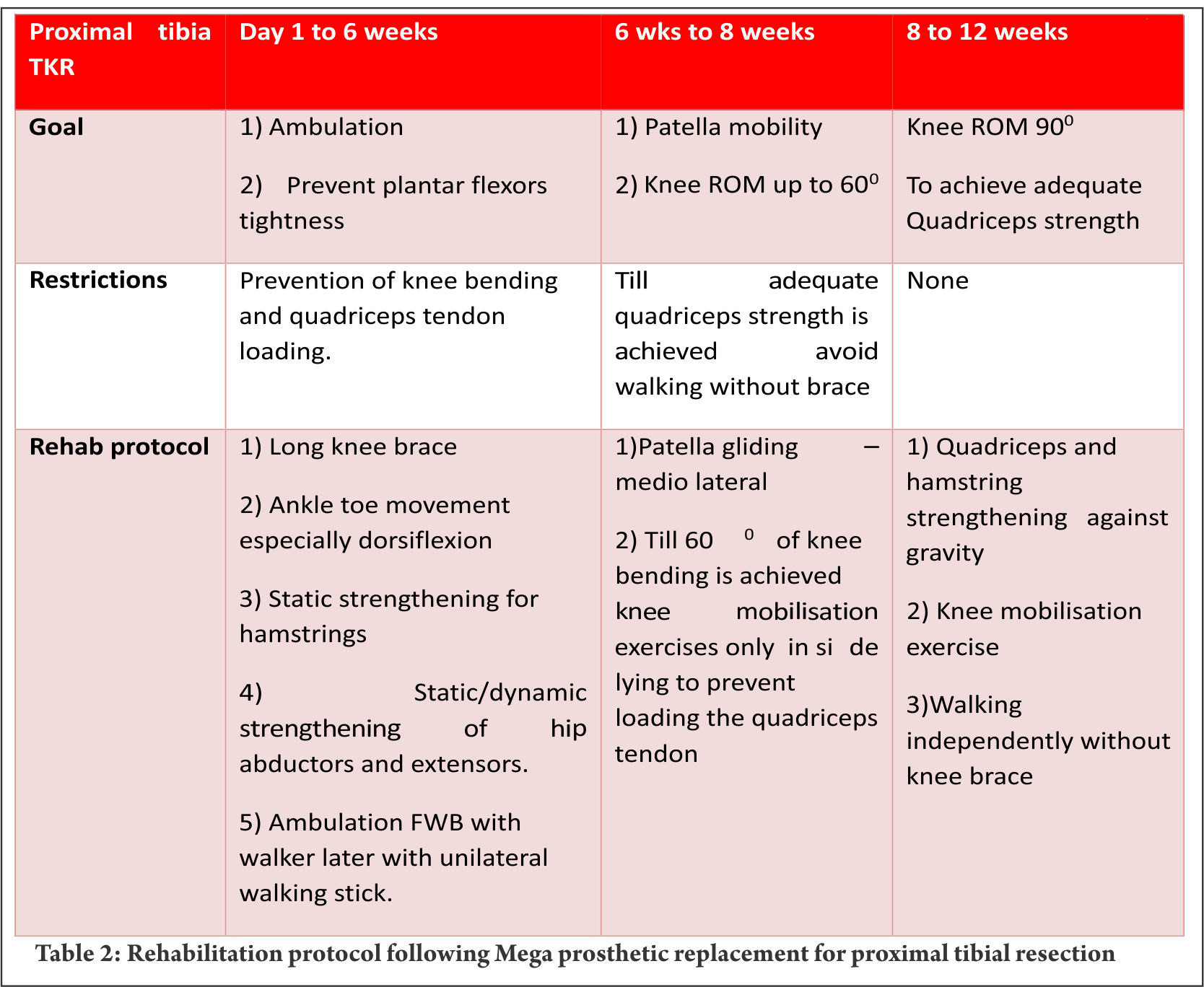
Proximal tibia and knee joint is the second most common site for primary high grade sarcoma and giant cell tumors. It is indeed a challenging location for rehabilitation in view of the fact that the extensor mechanism have to be reconstructed in these cases [4]. In most of the cases a gastrocnemius flap is done to provide a dynamic anchorage and direct anchorage to prosthesis provide a static attachment to help reattaching extensor mechanism to proximal tibial prosthesis. Protecting the extensor mechanism reconstruction till it attaches through fibrosis along with the surrounding soft tissue structures are crucial to prevent quadriceps lag. Hence, knee bending and quadriceps strengthening will be delayed for six weeks until then the knee is protected with the help of long knee brace. Re-attached gastrocnemius flap could lead to protective muscle spasm of plantar flexors and if not mobilised early it may create plantar flexors contracture. Thus, achieving/maintaining dorsi flexion of the ankle joint in the early post operative period is crucial for appropriate weight bearing. Mobilisation of knee joint and quadriceps strengthening could be started after six weeks; however, therapist must consider that immobilisation of the knee joint in long knee brace leads to severe restriction of patella mobility. Unless adequate patella mobility is achieved, especially the medial lateral movement, knee flexion exercises could prevent smooth gliding of patella over the femoral condyle. This will increase strain on the reconstructed patella ligament. Therefore, our institute follows a unique mobilisation protocol following proximal tibia and knee replacement which is depicted in the Table 2. In few cases quadriceps lag could be evident due to patella tendon overstretch/avulsion, this could be due to improper patella mobilisation or forceful knee bending. Fig. 3 a, b and c depicts the patella tendon overstretch.
Mega prosthetic replacement for proximal and total femoral resection:
Resection of proximal femur and prosthetic replacement may be done for proximal femur tumor or as a part of total femoral resection and reconstruction. Partial or complete loss of joint capsule and dynamic stabilisers of hip joint during tumor resection may leave the hip joint vulnerable to dislocation. This may get potentiated with certain combination movements, if these joint movements are allowed beyond a certain limit. This restriction largely depends upon the surgical approach. Postero-lateral approach being most common in the LSS of this site, hip rotations, especially internal rotation and, flexion more than 600 and adduction of the hip joint needs to be prevented up to 6 weeks [4,7]. These movement restrictions could be achieved using hip abduction pillow/brace and de-rotation splint. Before the patient gets discharged from the hospital, training them for bed transfer, supine to standing, standing to supine and sitting in a chair/commode becomes paramount important in the early phase of rehabilitation. Knee joint mobilisation must be started early either by the edge of bed with hip joint well supported or in side lying with pillows between legs. Any restriction of knee joint range would adversely affect the overall function since hip joint function of the ipsilateral leg has already been compromised. Early FWB ambulation could be started from post operative day one initially with walker, then with walking stick. Later most of them would be trained to walk without any walking aid. Total femoral resections may require more intense rehabilitation with additional emphasis on knee strengthening as discussed earlier (Table 2). Patients may life long need to use walking aids in view of the fact that large motor loss in these cases.
Mega prosthetic replacement for proximal humeral resections:
Proximal humerus and the shoulder girdle are the third common place for primary bone sarcomas [4]. Despite endoprosthetic replacements for functional shoulder girdle structures, such as reverse glenoid prosthesis, are available, lack of muscular structures post excision and damage to the axillary nerve often prevent their use. Frequently, the proximal end of the humerus is replaced with the endoprosthesis and suspended by the remaining muscles and soft tissue structures by suturing around the proximal end of the prosthesis. The objective of the procedure is to achieve a stable shoulder to facilitate good elbow and hand function.
To prevent the weight of the endoprosthesis and the limb acting on the newly formed pseudo joint, shoulder sling and elbow pouch are provided for 4 – 6 weeks. Early post operative rehabilitation consists of elbow and hand range of motion (ROM) and strengthening exercises within pain limit. Again these exercises must be performed in supine position only to avoid undue stress on the shoulder. After six weeks, shoulder joint limited ROM exercise in the form of pendular movements and vigorous strengthening of shoulder girdle, elbow and hand complex should be commenced. Additionally, postural correction must be included in the rehabilitation program.
Biological reconstructions
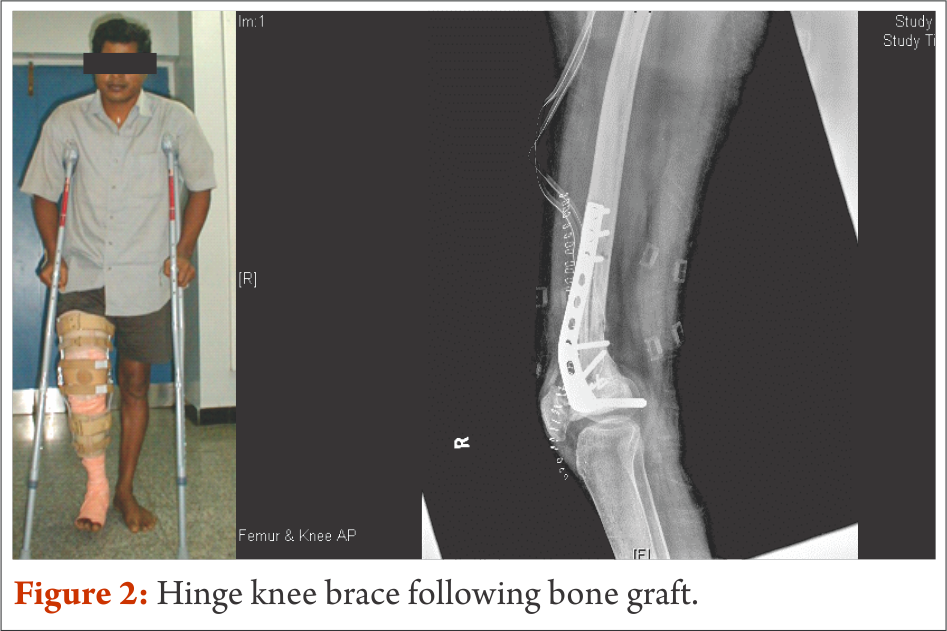
Wherever feasible, biological reconstructions are preferred over endoprosthetic implants in order to provide a stable and permanent solution for reconstruction of defects after tumor resection. However, rehabilitation following biological reconstructions needs careful considerations regarding weight bearing and joint mobilization. Utmost importance to surgical notes and communication with operative surgeon is of prime importance. Early joint mobilisation is the key to prevent joint stiffness and functional loss; nevertheless, often protective functional braces may be required to prevent damage. For example, curettage and bone grafting of the lower end of femur close to the joint demands hinge knee brace to avoid varus and valgus stress. Strengthening exercises also could be started early with functional knee brace (Fig. 4).
Patients are taught to walk non-weight bearing with brace generally from post operative day one with the help of axillary crutches up to 8 weeks. Once, osteosynthesis is confirmed through radiological evaluation, progressive weight bearing walking could be started. FWB walking and complete joint range and strength are expected to be achieved by the end of 3 months to 4 months.
conclusions
Although limb salvage surgery for primary malignant tumours have achieved commendable advancement in surgical techniques and endo-prosthetic design and manufacturing, without optimal and timely peri and post-operative physical rehabilitation, achieving the desired quality of life outcome may not be feasible. This paper has highlighted few important rehabilitation principles and we have summarised rehabilitation protocol for specific area. Most of the oncology resection and reconstruction vary from one individual to another even in one particular site and needs tailor made rehabilitation protocol; nevertheless, this summary will be a guide for necessary foundation to design individual rehabilitation program.
References
1. Chopra BK. Health related quality of life studies in Indian patients after limb salvage surgery: Need of the hour. Med J Armed Forces India. 2013 Jul;69(3):209–10.
2. Ottaviani G, Robert RS, Huh WW, Palla S, Jaffe N. Sociooccupational and physical outcomes more than 20 years after the diagnosis of osteosarcoma in children and adolescents. Cancer. 2013;119(20):3727–36.
3. Frieden RA, Ryniker D, Kenan S, Lewis MM. Assessment of patient function after limb-sparing surgery. Arch Phys Med Rehabil. 1993 Jan;74(1):38–43 6p.
4. Oren R, Zagury A, Katzir O, Kollender Y, Meller I. Principles of rehabilitation after limb-sparing surgery for cancer. In: Musculoskeletal Cancer Surgery [Internet]. Springer; 2001 [cited 2014 Sep 3]. p. 583–93. Available from: http://link.springer.com/chapter/10.1007/0-306-48407-2_36
5. Bekkering WP, Vliet Vlieland TPM, Fiocco M, Koopman HM, Schoones JW, Nelissen RGHH, et al. Quality of life, functional ability and physical activity after different surgical interventions for bone cancer of the leg: A systematic review. SurgOncol. 2012 Jun;21(2):e39–47.
6. Mei J, Zhu X-Z, Wang Z-Y, Cai X-S. Functional outcomes and quality of life in patients with osteosarcoma treated with amputation versus limb-salvage surgery: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2014 Nov;134(11):1507–16.
7. Shehadeh A, Dahleh ME, Salem A, Sarhan Y, Sultan I, Henshaw RM, et al. Standardization of rehabilitation after limb salvage surgery for sarcomas improves patients’ outcome. HematolOncol Stem Cell Ther. 2013 Sep;6(3–4):105–11.
8. Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc. 2010 Jul;42(7):1409–26.
9. Singh F, Newton RU, Galvão DA, Spry N, Baker MK. A systematic review of pre-surgical exercise intervention studies with cancer patients. SurgOncol. 2013 Jun;22(2):92–104.
10. Silver JK. Cancer Prehabilitation and its Role in Improving Health Outcomes and Reducing Health Care Costs. SeminOncolNurs. 2015 Feb;31(1):13–30.
11. Silver JK. Cancer prehabilitation and its role in improving health outcomes and reducing health care costs. SeminOncolNurs. 2015 Feb;31(1):13–30.
(Abstract Full Text HTML) (Download PDF)
Like this:
Limb Salvage With Megaprosthesis In Extremity Osteosarcoma –a Case-based Approach
Volume 2 | Issue 2 | May-Aug 2016 | Page 13-19 | Gurpal Singh, Mark Edward Puhaindran.
Authors: Gurpal Singh[1], Mark Edward Puhaindran[1].
[1]Orthopedic Oncology Services, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai.
Address of Correspondence
Division of Musculoskeletal Oncology, University Orthopaedics, Hand and Reconstructive Microsurgery Cluster, National University Health System, Singapore.
Abstract
Introduction: Musculoskeletal oncology is an evolving field in orthopaedic surgery and surgical management for patients with osteosarcoma has changed fundamentally over the past three decades. Osteosarcoma is a rare tumour, but it is the most common type of primary bone cancer with a biomodal peak. Primary cases tend to occur within the first two decades of life and secondary osteosarcomas affect older patients. Common causes of secondary osteosarcoma include Paget’s disease of bone and radiation exposure. Due to advances in chemotherapeutic regimes, imaging modalities, surgical techniques, material and prosthesis designs, amputation is no longer considered as treatment of choice for most patients. Limb salvage surgery including endoprosthetic reconstructions is also constantly evolving, addressing surgical challenges such as margin control, reconstructive procedures and soft tissue management. In this review, we focus our discussion on the management of patients with osteosarcoma undergoing megaprosthetic reconstruction. Based on three real cases (osteosarcoma of the distal femur, pelvic osteosarcoma involving the hip joint and osteosarcoma of the proximal tibia), this paper aims to highlight surgical challenges that sometimes need to be overcome in this very challenging field.
Keywords: Limb salvage surgery; megaprosthetic reconstruction; osteosarcoma; musculoskeletal oncology.
Introduction
Musculoskeletal oncology is a rapidly evolving field in orthopaedic surgery and surgical management for patients with osteosarcoma has progressed significantly over the past three decades. Due to advances in neoadjuvant treatment, imaging modalities, surgical techniques and material and prosthesis designs, amputation is no longer considered as standard of care in most cases. Literature is currently reporting limb salvage surgeries in 85% to 95% without compromising oncological principles when compared to amputation [1–5]. Main objectives of limb salvage surgery include maximized functional outcome, satisfactory wound coverage for adjuvant therapy and optimized aesthetic outcome without compromising oncologic principles [6]. The reconstructive options for limb salvage surgery can be thought of as biological (autograft, allograft etc.) or endoprosthetic. Sometimes, a combination of both may be necessary. When considering treatment options for patients with osteosarcoma, several factors need to be considered, including the response to neoadjuvant chemotherapy, evidence of periprosthetic fracture, anatomic site, involvement of soft tissue, joint and neurovascular structures as well as the evidence of metastases at diagnosis. Adequate margin control during surgery is crucial. Surgery represents only one component of the multidisciplinary treatment protocol of osteosarcoma patients. Since the 1970s, the role of neoadjuvant therapy has evolved and intense multi-agent chemotherapy has improved the prognosis significantly by eradicating accompanying micrometastases and also reducing the reactive zone around the tumour. The main drawback of chemotherapy prior to surgery includes immunosuppression. Therefore, a multidisciplinary approach between medical oncologists and the surgical team is essential in order to optimise treatment for the patient. After completion of neoadjuvant chemotherapy, re-staging is performed to assess response to chemotherapy and verify resectability and evaluate margins prior to proceeding with definite surgery. Limb salvage surgery for osteosarcoma is typically described as consisting of three parts, starting with en bloc resection of the tumour. Based on the exact location, intra- or extra-articular resection may be considered. In skeletally immature patients, the possibility of physis preservation should be considered. Thereafter, the bone defect is reconstructed. The third part of the surgery consists of soft tissue coverage and functional re-establishment. Treatment protocols for osteosarcoma further include the administration of adjuvant chemotherapy and subsequent long-term surveillance. After limb salvage surgery, overall survival rates of 60% to 70% at 5 years have been reported in literature [1–4, 9, 15]. A recent systematic review and meta-analysis by Stokke et al. evaluating the quality of life among paediatric, adolescent and young adult bone tumour survivors suggested that quality of time improves over time. According to their results, female patients and patients at older age are more likely to have a poor quality of life. Interestingly, there was no difference in outcomes between patients who underwent limb salvage surgery versus amputation for local control [16]. Failure rates in patients undergoing reconstruction with megaprostheses are generally higher compared to patients treated with conventional arthroplasties [7]. However, a direct comparison of study findings is difficult due to different settings and definitions used. Failure rates between 40% to 73% at 5 to 15 years have been reported from factors due to the underlying disease contributing to unfavourable early and late surgical outcome, complications can be specifically related to endoprosthetic reconstruction including aseptic loosening, periprosthetic fracture, infection, implant failure, dissociation of modular components and wear [1, 2, 5, 8, 9]. Implant survival rates for fixed-hinge prostheses have been reported to be approximately 70%, whereas rotating hinge prostheses survival between almost 80 to 100% have been reported [1, 7, 10–13]. A classification system proposed by Henderson et al. for megaprosthesis failure indicates 5 causes of failure, including soft tissue failure (Type 1), aseptic loosening (Type 2), structural fracture (Type 3), infection (Type 4) and local tumour recurrence (Type 5) [14].
Three case examples of patients with osteosarcoma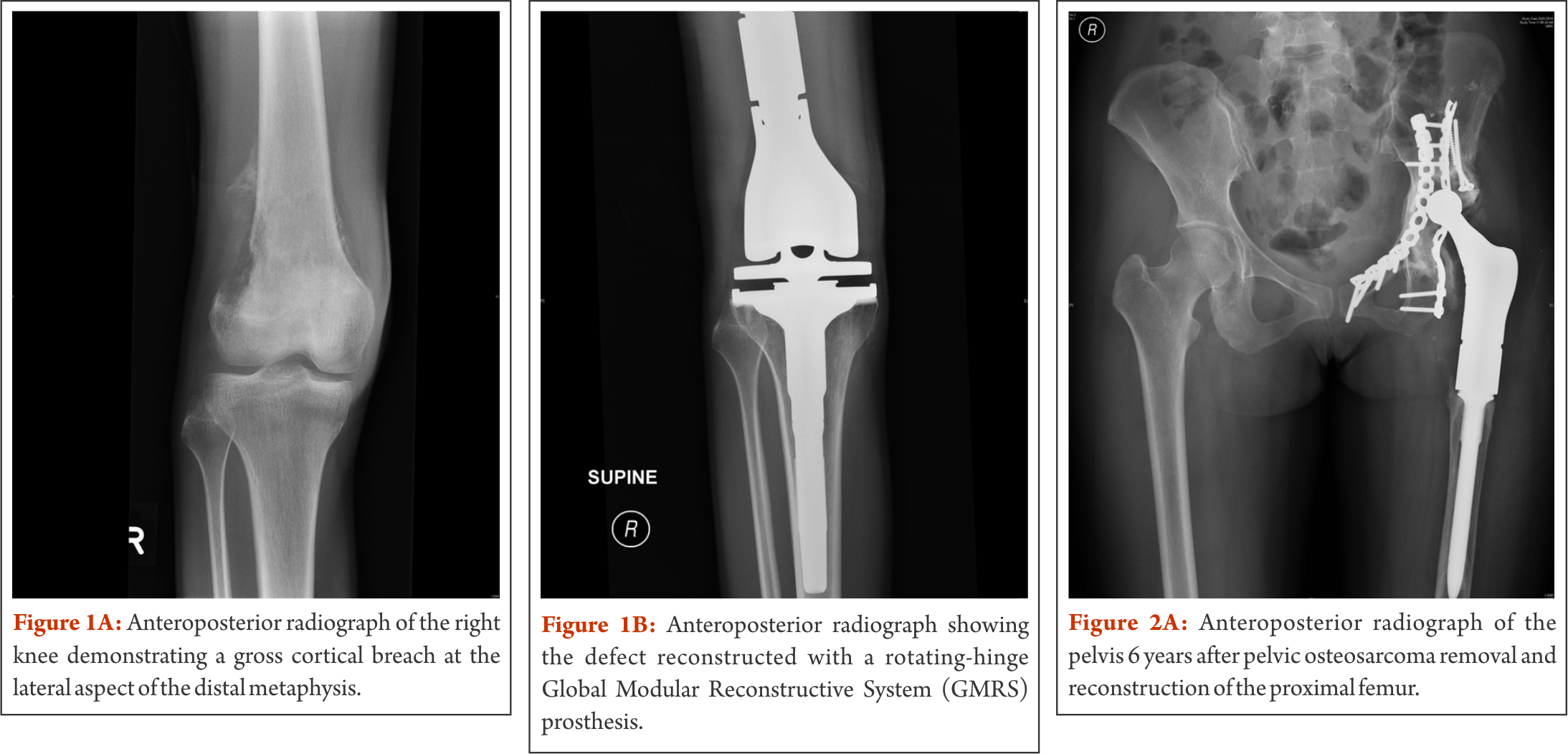
Case 1 – Osteosarcoma of the distal femur
A 16 year old male patient presented with right knee pain at the lateral aspect of the knee and night pain for about one month. There was no known trauma to the right knee. Clinical findings revealed tenderness over the medial and lateral aspect of the knee and a decreased range of motion 10-110°. Plain radiograph, magnetic resonance imaging, computed tomography and bone scan for local and distal staging were performed, showing an aggressive right distal femoral tumour, with extraosseous soft tissue extension abutting the quadriceps and gastrocnemius muscles, iliotibial band, and medial and lateral gutters of the knee joint (Figure 1a). No fracture or neurovascular involvement was detected. There was no evidence of distant osseous or pulmonary metastases. An open biopsy confirmed the diagnosis of a high-grade conventional osteosarcoma.
After completion of neoadjuvant chemotherapy, the patient developed an extensive local fungal infection on the lateral aspect of the thigh, surrounding the biopsy incision site. Systemic antifungal therapy was given for two weeks, directed by a dermatologist and surgery was delayed by two weeks. Given the small window of opportunity between neoadjuvant and adjuvant chemotherapy and to minimise further delay in treatment, the surgical team in the outlined case decided to proceed with tumour resection. In view of the recent tinea corporis with lesions on the lateral aspect of the right thigh, the decision was made to proceed with an anteromedial approach with the excision of the biopsy tract laterally. Local tumour recurrence as a result of spread of malignant cells during biopsy has been reported [17, 18]. Consequently, the biopsy tract is considered as contaminated and conventionally excised during tumour removal. However, more recent studies have shown preliminary evidence for the safety of limb salvage surgery without biopsy tract excision following a diagnostic core needle biopsy and fine-needle aspiration, respectively [19, 20]. In the outlined case, a medial dissection via interval between vastus medialis and rectus femoris was performed for en bloc resection of the tumour. Femoral vessels were identified and traced into the popliteal fossa via adductor canal. The femur osteotomy was made at pre-templated 150 mm from the joint line. The sciatic and peroneal nerve were identified and preserved. Histopathological analysis of frozen sections and tumour specimen showed negative margins. After change of instruments, distal femur reconstruction was continued. Femur and tibia were prepared and a rotating-hinge Global Modular Reconstructive System (GMRS) (Stryker Inc, Rutherford, NJ, USA) knee prosthesis was used for reconstruction (Figure 1b). The vastus medialis was mobilised and brought down to cover the defect medially. The extensor mechanism was reconstructed over the prosthesis. No post-operative complications occurred, all wounds healed satisfactorily. Six months after surgery, the patient is walking without any support. This case highlights the necessity of non-conventional surgical approaches when necessary. Although the main tumour burden was on the lateral aspect of the knee joint, given the location of the previous treated fungal infection, the decision for a medial approach was made. Extra- versus intraarticular resection needs to be discussed in the appropriate context. Preliminary evidence is hinting towards an overestimation of neoplasm seeding in the biopsy tract, especially when the biopsy is performed by the operating surgeon himself. The point to emphasize in this case is the close communication between medical oncologist and the surgeon and balancing the risks of delaying adjuvant chemotherapy versus an “unconventional” surgical approach. This patient underwent an intraarticular resection of the distal femur. In cases where the knee joint is found to be contaminated or being directly invaded by the tumour, an extraarticular resection of the entire joint with en-bloc removal is recommended. Usually, this approach is associated with poorer functional results.
Case 2 – Pelvic osteosarcoma involving the hip joint
A 24 year old female patient presented with a left neck of femur fracture with underlying osteosarcoma. Prognostic and treatment implications of pathological fractures at presentation have been widely debated. In the past, pathological fractures have been considered as indication for amputation due to the risks of local recurrence from contamination caused by the fracture hematoma. However, a recent systematic review and meta-analysis by Salunke et al. is demonstrating similar rates of local recurrence in patients with limb salvage surgeries compared to amputation, provided carefully selection of patients has been performed [21]. Our own 18-year experience of high-grade osteosarcoma with a pathological fracture at initial presentation showed no differences in the survival and recurrence rates of patients with pathological fractures compared to those with no fractures. Moreover, we did not see any difference in survival between amputated and salvaged patients with fractures, provided margin control attempts are aggressive (unpublished data). In the outlined case, the patient was treated according to protocol with neoadjuvant chemotherapy. Given the complexity of the case, but still aiming for limb salvage, the decision was made for using endoprosthetic and biologic reconstructive options, namely the combination of a hemipelvectomy with an extra-articular proximal femur resection followed by proximal femur replacement and acetabular column plating/deep frozen bone (Fig. 2a). Biologic reconstruction options such as allografts, autografts and re-implantation of sterilized tumour bone replace the defect with a biologic construct, providing the theoretical advantage of incorporation of the biological graft. However, retrieval studies have shown that grafts become necrotic and may act as a spacer rather than a stable replacement. Typical failures include graft-fracture, non-union between the graft and host-bone and increased infection-rates. Drawbacks also include the dependence of graft incorporation for rehabilitation. A reliable tissue bank and associated logistics are sine qua non, and harvesting the autograft or preparing the allograft and subsequently increasing surgical time need to be taken into account. Since a long-term study showed that less than 50% of allografts lasted less than 10 years [22], this technique is mostly preserved for special occasions only, such as osteosarcomas in skeletally immature patients without involving the growth plates. Combined usage of endoprosthetic and biologic reconstruction is described by the allograft prosthetic composite. The concept behind includes restoration of the bone stock by allograft and using endoprosthetic components to restore articulating surfaces, theoretically offering a higher durability in the long-term when compared to pure biologic reconstruction. In the outlined case, the patient’s own pre-treated tumour bone was used for part of the recontruction. Sterilization of the bone can be performed in various ways including pasteurizing, autoclaving, radiotherapy, and freezing. Similarly to the use of allografts, non-union, infection and fracture belong to the main complications in biologic reconstruction with autografts. As described in the outlined case, liquid nitrogen was used for pre-treatment of the bone. Cryosurgery in combination with autograft-prosthesis composites shows promising results with excellent functional outcomes, low complication rates and improved union rates, especially when used with the pedicle-freezing technique [23–25]. After completion of adjuvant chemotherapy and being in remission, the patient in the outlined case developed a hematogenous methicillin susceptible staphylocococcus aureus (MSSA) infection of the endoprosthesis six years postoperatively. Infection is still the most common complication in megaprosthetic reconstruction and in general, it is more likely to happen when adequate wound coverage is missing. In primary megaprosthesis infection rates between 2% to 20% have been reported, with the numbers increasing to more than 40% in revision cases [1, 2, 5, 10, 14, 26–31]. The classic approach in periprosthetic infection is a two-stage exchange revision surgery, including the removal of original endoprosthetic components, thorough debridement, administration of intravenous antibiotics, and implantation of a spacer followed by the re-implantation of implants. In the outlined case, this approach was not practical. A consensus with the multidisciplinary musculoskeletal oncology team and the patient was made for management with ultrasound-guided drainage of the left hip joint and suppressive antibiotics with follow-ups by our colleagues for infectious disease. The patient was discharged with peripherally inserted central catheter line in situ. She continued to develop a collection in the left hip and anterior thigh. A formal arthrotomy with extensive debridement and removal of all necrotic tissue was performed. A large bore chest drain was left in situ, exited through quadriceps anteriorly, plus two additional drains subcutaneously. An urostomy pouch was applied and the patient was kept on long term drainage, allowing the sinus track to the left lateral thigh to mature. In the following, kept with suppressive antibiotics (ciprofloxacin and rifampicin), the patient was under close follow-up with a regular change of the urostomy bag. Erythema and tenderness regressed and drainage successively decreased (Figure 2b). The chest drain was removed two months after surgery. On examination, 29 months after debridement the left thigh is non-tender and showed no erythema. Scars to the left tight (sinus track) are well healed and she had no fever, chills or rigor and denied any pain. She is walking with a slight limp and was returned to work recently. She remains on long-term suppressive antibiotics as guided by the infectious disease physician. This case highlights how limb salvage surgery has pushed the boundaries over the last decades. Combining different reconstructive options may be considered for complex cases. This case also illustrates the option of a relatively conservative management strategy for periprosthetic infection in a compliant patient, achieving a satisfactory result.
Case 3 – Osteosarcoma of the proximal tibia
A 16 year old female patient was diagnosed with non metastatic osteosarcoma of the left proximal tibia (stage IIb). She underwent left tibial osteosarcoma resection, reconstruction with megaprosthesis, extensor mechanism reconstruction, medial gastrocnemius flap and split skin graft (Figure 3a and 3b). Proximal tibia resection presents unique local anatomical features which need to be addressed during limb salvage surgery. Neurovascular structures in the popliteal fossa as well as the peroneal nerve between the biceps femoris and the lateral head of the gastrocnemius muscle need to be preserved as much as possible. Displacement of these structures due to a large tumour mass are likely, therefore careful preparation in this area is required. In most cases, biological borders such as perivascular fat or the popliteus muscle are separating the tumour from the neurovascular bundle. Intraoperatively, overstretching these structures due to overdistraction of the femur and tibia (after resecting the tumour) needs to be avoided in order to prevent neuropraxia and endothelial injury. Involvement of tissue adjacent to the tibiofibular joint is usually of concern and this joint is typically included in the resection. Once the patellar tendon has been divided, reconstruction of the extensor mechanism is obligatory. Various techniques to attach the tendon to the endoprostetic implant have been described in a systematic review by Ek et al. including direct fixation using screw/washer or sutures, synthetic soft tissue augments such as tubes, sutures, cerclage wires and non-absorbable tapes and biological augmentation such as graft from the biceps or satorius tendons or gastrocnemius flaps with or without synthetic materials [32]. The authors report a trend towards improved outcomes with biologic reconstructive options. However, there is no clear evidence for a single technique. Extensor lag is of major concern in all surgeries requiring reconstruction of the extensor mechanism. Therefore, postoperative management in the outlined case included immobilization with a long-leg cast and a long-leg brace respectively for six weeks to allow healing. Obtaining full extension and allowing the extensor mechanism to heal was given priority compared to knee flexion in view of its impact on ambulation and there was a strong emphasis on extensor mechanism strengthening during rehabilitation. The close proximity of the proximal tibia to the skin makes the wound more susceptible to infectious complications. Keeping thick flaps during preparation at the beginning of the surgery minimize necrosis of the skin. Typically, a primary medial gastrocnemius flap is used to improve wound coverage with the advantage of offering a larger muscular material and also bypassing a longer distance when compared to the lateral gastrocnemius [33, 34]. This technique has been first described by Dubousset et al. [35]. Skin grafting provides an additional supportive procedure while relieving tension during skin closure and therefore preventing skin flap necrosis. Currently, split-thickness skin graft is considered as gold standard in any major skin loss. Typically, the graft is meshed in order for expansion while keeping the morbidity to the donor side as low as possible. Postoperative management in patients with skin grafts includes a close observation of the donor side for scarring, pain and signs suggestive of infection. This case illustrates a conventional proximal tibia resection, highlighting surgical considerations with regards to anatomical characteristics and postoperative management.
conclusions
Medical management, surgical techniques and prosthetic design have improved significantly during the last three decades. Amputation is no longer considered as standard of care in patients with osteosarcoma in most cases. However, limb salvage with megaprosthesis remains challenging. Complication rates are high, with infection occurring most commonly. A good interaction within a multidisciplinary team in a preferably high-volume centre is required for optimal management. Given the unique features of these patients, “unconventional” approaches and combinations of reconstructive options may be considered sometimes, provided oncologic principles are not compromised.
References
1.Pala E, Trovarelli G, Calabrò T, Angelini A, Abati CN, Ruggieri P. Survival of modern knee tumor megaprostheses: failures, functional results, and a comparative statistical analysis. Clin Orthop Relat Res 2015;473:891–9.
2.Zeegen EN, Aponte-Tinao LA, Hornicek FJ, Gebhardt MC, Mankin HJ. Survivorship analysis of 141 modular metallic endoprostheses at early followup. Clin Orthop Relat Res 2004:239–50.
3.Bacci G, Ferrari S, Bertoni F, Ruggieri P, Picci P, Longhi A, et al. Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the istituto ortopedico rizzoli according to the istituto ortopedico rizzoli/osteosarcoma-2 protocol: an updated report. J Clin Oncol 2000;18:4016–27.
4.Bacci G, Picci P, Ferrari S, Ruggieri P, Casadei R, Tienghi A, et al. Primary chemotherapy and delayed surgery for nonmetastatic osteosarcoma of the extremities. Results in 164 patients preoperatively treated with high doses of methotrexate followed by cisplatin and doxorubicin. Cancer 1993;72:3227–38.
5.Gosheger G, Gebert C, Ahrens H, Streitbuerger A, Winkelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res 2006;450:164–71.
6.Heller L, Kronowitz SJ. Lower extremity reconstruction. J Surg Oncol 2006;94:479–89. doi:10.1002/jso.20485.
7.Heisel C, Kinkel S, Bernd L, Ewerbeck V. Megaprostheses for the treatment of malignant bone tumours of the lower limbs. Int Orthop 2006;30:452–7.
8.Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol 2013;107:335–42.
9.Orlic D, Smerdelj M, Kolundzic R, Bergovec M. Lower limb salvage surgery: modular endoprosthesis in bone tumour treatment. Int Orthop 2006;30:458–64.
10.Ahlmann ER, Menendez LR, Kermani C, Gotha H. Survivorship and clinical outcome of modular endoprosthetic reconstruction for neoplastic disease of the lower limb. J Bone Joint Surg Br 2006;88:790–5.
11.Bhangu AA, Kramer MJ, Grimer RJ, O’Donnell RJ. Early distal femoral endoprosthetic survival: cemented stems versus the Compress implant. Int Orthop 2006;30:465–72.
12.Myers GJC, Abudu AT, Carter SR, Tillman RM, Grimer RJ. Endoprosthetic replacement of the distal femur for bone tumours: long-term results. J Bone Joint Surg Br 2007;89:521–6. doi:10.1302/0301-620X.89B4.18631.
13.Ruggieri P, Mavrogenis AF, Pala E, Abdel-Mota’al M, Mercuri M. Long term results of fixed-hinge megaprostheses in limb salvage for malignancy. Knee 2012;19:543–9.
14.Henderson ER, Groundland JS, Pala E, Dennis JA, Wooten R, Cheong D, et al. Failure mode classification for tumor endoprostheses: retrospective review of five institutions and a literature review. J Bone Joint Surg Am 2011;93:418–29.
15.Eckardt JJ, Eilber FR, Dorey FJ, Mirra JM. The UCLA experience in limb salvage surgery for malignant tumors. Orthopedics 1985;8:612–21.
16.Stokke J, Sung L, Gupta A, Lindberg A, Rosenberg AR. Systematic review and meta-analysis of objective and subjective quality of life among pediatric, adolescent, and young adult bone tumor survivors. Pediatr Blood Cancer 2015;62:1616–29.
17.Schwartz HS, Spengler DM. Needle tract recurrences after closed biopsy for sarcoma: three cases and review of the literature. Ann Surg Oncol 1997;4:228–36.
18.Davies NM, Livesley PJ, Cannon SR. Recurrence of an osteosarcoma in a needle biopsy track. J Bone Joint Surg Br 1993;75:977–8.
19.Saghieh S, Masrouha KZ, Musallam KM, Mahfouz R, Abboud M, Khoury NJ, Haidar R. The risk of local recurrence along the core-needle biopsy tract in patients with bone sarcomas. Iowa Orthop J 2010;30:80–3.
20.Kaffenberger BH, Wakely PE, Mayerson JL. Local recurrence rate of fine-needle aspiration biopsy in primary high-grade sarcomas. J Surg Oncol 2010;101:618–21.
21.Salunke AA, Chen Y, Tan JH, Chen X, Khin LW, Puhaindran ME. Does a pathological fracture affect the prognosis in patients with osteosarcoma of the extremities?: A systematic review and meta-analysis. Bone Joint J 2014;96-B:1396–403. doi:10.1302/0301-620X.96B10.34370.
22.Brigman BE, Hornicek FJ, Gebhardt MC, Mankin HJ. Allografts about the Knee in Young Patients with High-Grade Sarcoma. Clin Orthop Relat Res 2004:232–9.
23.Subhadrabandhu S, Takeuchi A, Yamamoto N, Shirai T, Nishida H, Hayashi K, et al. Frozen Autograft-Prosthesis Composite Reconstruction in Malignant Bone Tumors. Orthopedics 2015;38:e911-8.
24.Jeon D, Kim MS, Cho WH, Song WS, Lee S. Pasteurized autograft-prosthesis composite for distal femoral osteosarcoma. J Orthop Sci 2007;12:542–9. doi:10.1007/s00776-007-1173-7.
25.Jeon D, Kim MS, Cho WH, Song WS, Lee S. Pasteurized autograft-prosthesis composite for reconstruction of proximal tibia in 13 sarcoma patients. J Surg Oncol 2007;96:590–7.
26.Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, Gosheger G. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg 2006;126:289–96.
27.Lee SH, Oh JH, Lee KS, Yoo KH, Kim HS. Infection after prosthetic reconstruction in limb salvage surgery. Int Orthop 2002;26:179–84. doi:10.1007/s00264-001-0328-y.
28.Unwin PS, Cannon SR, Grimer RJ, Kemp HB, Sneath RS, Walker PS. Aseptic loosening in cemented custom-made prosthetic replacements for bone tumours of the lower limb. J Bone Joint Surg Br 1996;78:5–13.
29.Grimer RJ, Belthur M, Chandrasekar C, Carter SR, Tillman RM. Two-stage revision for infected endoprostheses used in tumor surgery. Clin Orthop Relat Res 2002:193–203.
30.Horowitz SM, Lane JM, Otis JC, Healey JH. Prosthetic arthroplasty of the knee after resection of a sarcoma in the proximal end of the tibia. A report of sixteen cases. J Bone Joint Surg Am 1991;73:286–93.
31.Jeys LM, Grimer RJ, Carter SR, Tillman RM. Periprosthetic infection in patients treated for an orthopaedic oncological condition. J Bone Joint Surg Am 2005;87:842–9. doi:10.2106/JBJS.C.01222.
32.Ek EW, Rozen WM, Ek ET, Rudiger HA. Surgical options for reconstruction of the extensor mechanism of the knee after limb-sparing sarcoma surgery: an evidence-based review. Arch Orthop Trauma Surg 2011;131:487–95.
33.McCraw JB, Fishman JH, Sharzer LA. The versatile gastrocnemius myocutaneous flap. Plast Reconstr Surg 1978;62:15–23.
34.Meller I, Ariche A, Sagi A. The role of the gastrocnemius muscle flap in limb-sparing surgery for bone sarcomas of the distal femur: a proposed classification of muscle transfers. Plast Reconstr Surg 1997;99:751–6.
35.Dubousset J, Missenard G, Genin J. Traitement chirurgical conservateur des sarcomes ostéogéniques des membres. Techniques et résultats fonctionnels. Rev Chir Orthop Reparatrice Appar Mot 1985;71:435–50.
(Abstract Full Text HTML) (Download PDF)
Like this: