Plantar Fibromatosis Masquerading as Liposarcoma : a Case Report and Review of Literature
Volume 2 | Issue 2 | May-Aug 2016 | Page 25-29 | Nishit Bhatnagar, Purushotham Lingaiah, Sumit Arora, Anil Dhal.
Authors: Nishit Bhatnagar [1], Purushotham Lingaiah [1], Sumit Arora [1], Anil Dhal [1].
[1]Department of Orthopaedic Surgery, Maulana Azad Medical College & associated Lok Nayak Hospital, New Delhi-110002
Address of Correspondence
Dr. Nishit Bhatnagar
7 Godavari Apartments, Alaknanda, New Delhi – 19
E-mail id: nishitbhatnagar@yahoo.co.in
Abstract
Plantar fibromatosis and well differentiated liposarcoma can have a similar clinical presentation of a slow growing superficial well defined mass on the plantar aspect of foot. We present a patient of plantar fibromatosis mimicking a lipomatous tumour of the foot. Marginal resection of the remaining tumour was performed. At two years postoperatively, there has been no recurrence of the tumour.
Keywords: liposarcoma, foot, plantar fibromatosis
Introduction
Plantar fibromatosis is a benign lesion involving the plantar aponeurosis. Ledderhose [1] in 1897 reported and described approximately 50 cases of contractures of the plantar fascia, leading to the entity being termed as Ledderhose’s disease. Its similarity to Dupuytrens’s disease of the hand has also led to the term “Dupuytren’s disease of the plantar fascia” [2]. It is commonly known to occur in the 3rd to 5th decade of life, has a male preponderance and is bilateral in 20 to 50% of cases [3,4,5]. It has an unknown etiology and is characterized by neoplastic proliferation of immature fibroblasts with spindle-shaped myofibroblasts within the plantar fascia [6]. They can be locally aggressive, demonstrate local recurrence but do not metastasize. Lipogenic tumours represent the most common soft tissue tumours [7]. Atypical and malignant lipomatous neoplasms are the most common variety of adult soft tissue sarcomas, accounting for nearly 20% of all sarcomas [8]. Lipomatous tumours are most frequently found in the extremities, retroperitoneum, groin and abdominal wall [9]. Lipomatous tumours can range from benign lipomas to highly malignant dedifferentiated liposarcomas [10]. Nomenclature and classification of lipomatous tumours has undergone major changes over time. Based on cytogenetic and molecular genetic studies, liposarcomas were classified by the World Health Organization Committee for classification of soft tissue tumours into five subtypes, atypical/well-differentiated liposarcoma, dedifferentiated liposarcoma, myxoid liposarcoma (including high grade round cell liposarcoma), pleomorphic liposarcoma and a rare mixed-type liposarcoma [8]. Some workers have proposed that the term ‘atypical lipomatous tumour’ should be used for tumours arising from extremities and chest wall, whereas ‘well differentiated liposarcoma’ should be used for describing tumours arising in the retroperitoneum and abdominal cavity [11,12,13]. Diagnosis of well differentiated liposarcomas of the extremities can be delayed due to relatively benign symptomatology and a low index of suspicion. Plantar fibromatosis and well differentiated liposarcoma can have a similar clinical presentation of a slow growing superficial well defined mass on the plantar aspect of foot. Here we present a patient of plantar fibromatosis mimicking a lipomatous tumour of the foot.
Case presentation
A 68-years-old male of Indian subcontinent was referred to our department with a ten year history of slow growing nodular masses on the non-weight bearing part of sole and along the lateral border of the right foot. The mass on the sole of the foot had become painful over the last one year. The masses were superficial, well defined, mildly tender and soft to firm in consistency (Fig. 1). 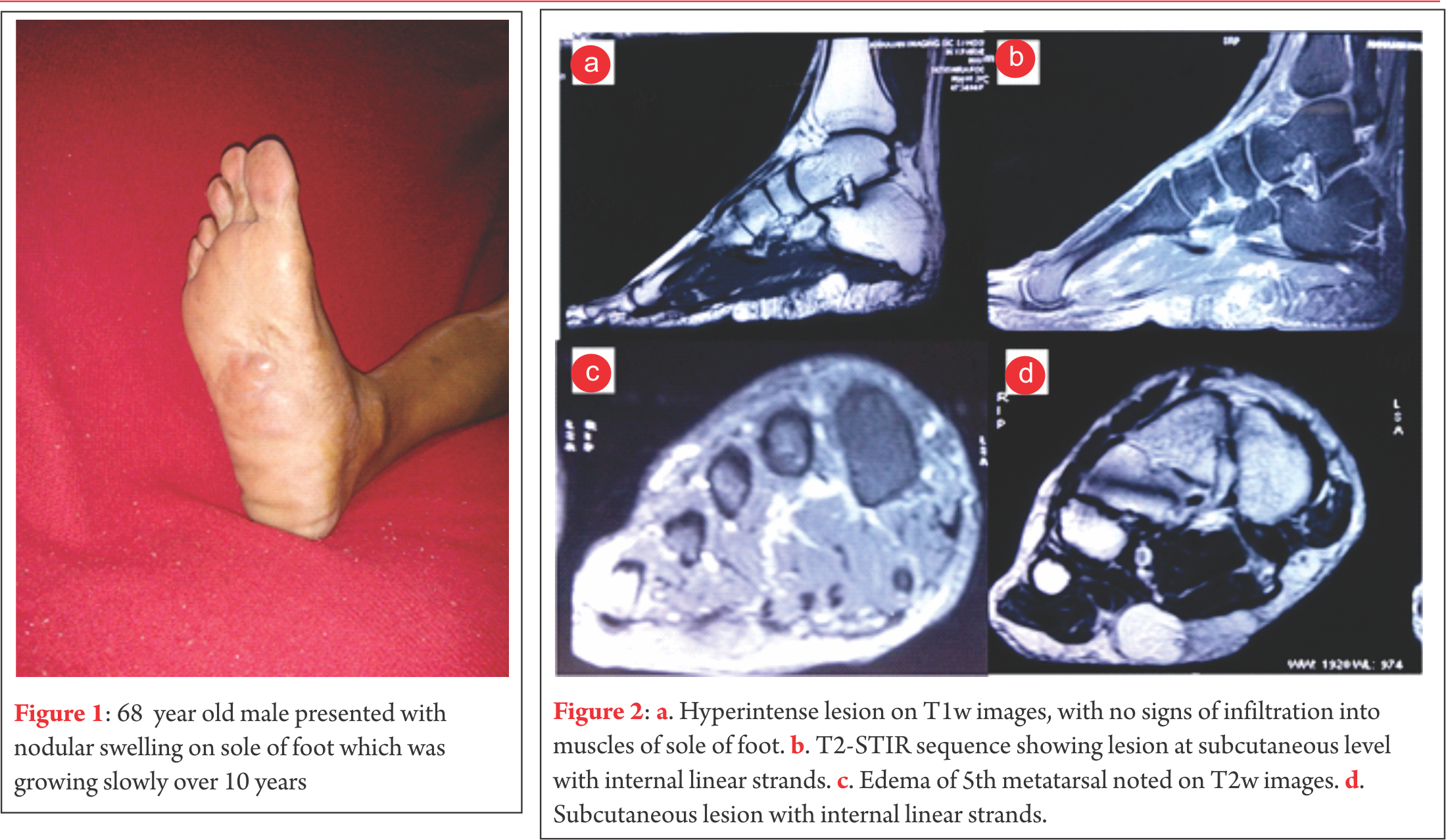 A diagnosis of plantar fibromatosis was made, keeping lipoma as a differential diagnosis. Plain radiographs showed no bony pathology. An unsuccessful trial of oral analgesics and customized insole was given. Prior to operative intervention for the mass on the plantar aspect of foot an excisional biopsy of the mass on the lateral border of the foot was performed. The biopsy revealed nodular non-encapsulated fibrofatty tissue on gross examination. Histopathological examination revealed nodular proliferation of adipocytes and myofibroblasts separated by collagenous bands. The nodules of fatty tissue showed a mixture of mature and immature fat cells with multivacuolation and nuclear indentation. Nuclear pleomorphism, hyperchromasia and mitosis were observed leading to a diagnosis of well differentiated liposarcoma. MRI revealed a 6.5cm x 6.6cm x 2cm well circumscribed, multilobulated lesion along the plantar aspect of the mid foot at the subcutaneous level that appeared to be indistinguishable from surrounding subcutaneous fat with internal linear strands. It was seen to insinuate between medial and lateral heads of plantar aponeurosis, however it did not show infiltration into the muscles of sole of the foot. Overlying skin of sole of foot appeared uninvolved. The lesion was hyperintense on T1w images, however suppresses completely on T2-STIR sequences. Few linear strands are noted tha are isointense in T1w images and showed enhancement in post contrast images (Fig. 2). Except for subtle focal edema in the base of the fifth metatarsal there was no bony involvement. Marginal resection of the remaining tumour was performed through an S-shaped incision on the non-weight bearing area of the sole. Tumour tissue was found to be lying between the dermis and the plantar aponeurosis. It was observed to be comprised of friable adipose tissue with a few intervening fibrotic septae. Tumor was non-encapsulated, however it could be easily separated from rest of the neighbouring structures. The adjacent aponeurosis and dermis appeared to be free of any gross tumour infiltration. The medial plantar neurovascular bundle also appeared free from any tumour infiltration. Histology revealed nodules of mature and immature adipose tissue separated by fibrovascular septae with areas of increased cellularity, pleomorphism, hyperchromasia and tumour giant cells (Fig. 3).
A diagnosis of plantar fibromatosis was made, keeping lipoma as a differential diagnosis. Plain radiographs showed no bony pathology. An unsuccessful trial of oral analgesics and customized insole was given. Prior to operative intervention for the mass on the plantar aspect of foot an excisional biopsy of the mass on the lateral border of the foot was performed. The biopsy revealed nodular non-encapsulated fibrofatty tissue on gross examination. Histopathological examination revealed nodular proliferation of adipocytes and myofibroblasts separated by collagenous bands. The nodules of fatty tissue showed a mixture of mature and immature fat cells with multivacuolation and nuclear indentation. Nuclear pleomorphism, hyperchromasia and mitosis were observed leading to a diagnosis of well differentiated liposarcoma. MRI revealed a 6.5cm x 6.6cm x 2cm well circumscribed, multilobulated lesion along the plantar aspect of the mid foot at the subcutaneous level that appeared to be indistinguishable from surrounding subcutaneous fat with internal linear strands. It was seen to insinuate between medial and lateral heads of plantar aponeurosis, however it did not show infiltration into the muscles of sole of the foot. Overlying skin of sole of foot appeared uninvolved. The lesion was hyperintense on T1w images, however suppresses completely on T2-STIR sequences. Few linear strands are noted tha are isointense in T1w images and showed enhancement in post contrast images (Fig. 2). Except for subtle focal edema in the base of the fifth metatarsal there was no bony involvement. Marginal resection of the remaining tumour was performed through an S-shaped incision on the non-weight bearing area of the sole. Tumour tissue was found to be lying between the dermis and the plantar aponeurosis. It was observed to be comprised of friable adipose tissue with a few intervening fibrotic septae. Tumor was non-encapsulated, however it could be easily separated from rest of the neighbouring structures. The adjacent aponeurosis and dermis appeared to be free of any gross tumour infiltration. The medial plantar neurovascular bundle also appeared free from any tumour infiltration. Histology revealed nodules of mature and immature adipose tissue separated by fibrovascular septae with areas of increased cellularity, pleomorphism, hyperchromasia and tumour giant cells (Fig. 3). 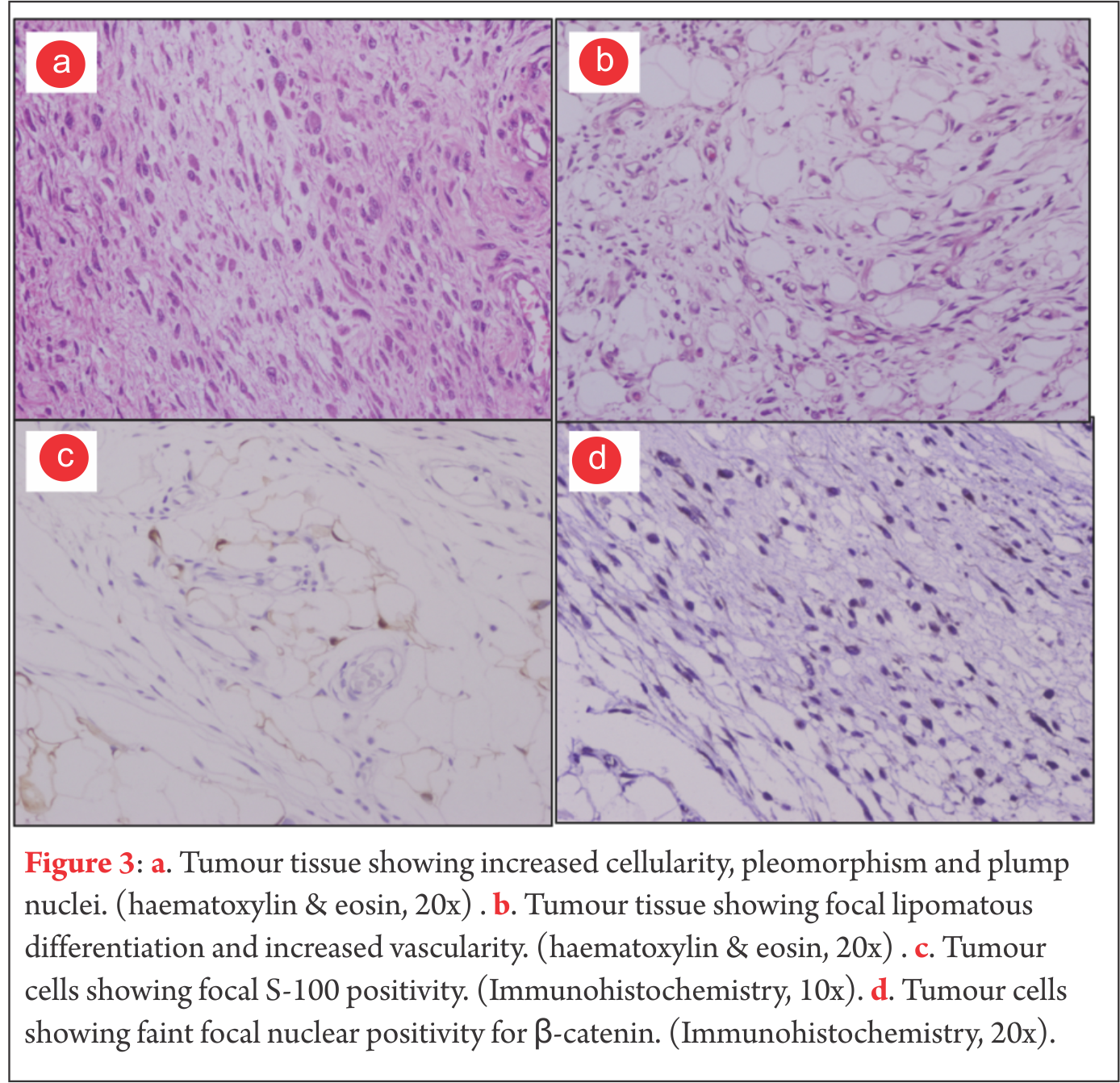 Mitotic figures were rare. Occasional cell with lipoblast like morphology was seen. Focal S-100 positivity was seen. Fatty tissue adherent to the skin also showed lesion cells in them. Due to proximity of tumour to the skin of the sole, thin skin flaps had to be created. Postoperatively marginal skin necrosis was observed and wound healing was delayed. Patient did not receive any postoperative chemotherapy or radiotherapy. At two years postoperatively, there has been no recurrence of the tumour and patient is able to ambulate without any discomfort. Patients consent was solicited before publishing the report
Mitotic figures were rare. Occasional cell with lipoblast like morphology was seen. Focal S-100 positivity was seen. Fatty tissue adherent to the skin also showed lesion cells in them. Due to proximity of tumour to the skin of the sole, thin skin flaps had to be created. Postoperatively marginal skin necrosis was observed and wound healing was delayed. Patient did not receive any postoperative chemotherapy or radiotherapy. At two years postoperatively, there has been no recurrence of the tumour and patient is able to ambulate without any discomfort. Patients consent was solicited before publishing the report
Discussion
Liposarcomas of the extremities are the second most commonly encountered soft tissue sarcoma after fibrous / fibrohistiocytic malignancies [14]. They occur almost exclusively in the age group between 40 to 60 years of age [14,15]. Liposarcomas are commonly encountered in the lower extremity, usually in the thigh, but rarely in the foot. Enzinger et al analyzed 1067 cases of liposarcoma, but none of them were in the foot [16]. There have been very few cases of liposarcomas of the foot reported in literature [17,18,19,20]. Preoperative diagnosis is infrequent. Hence, increasing the understanding of this tumour is important. WHO has categorized liposarcoma into five subtypes, out of which the well-differentiated variety is the most common, accounting for approximately 40% to 50% of all liposarcomas [21,14,22]. According to Evans et al a ‘well-differentiated liposarcoma’ and ‘atypical lipoma’ are identical in biological, behaviour, histological and karyotypic characteristics [23]. The term well differentiated liposarcoma is better used for lipomatous lesion in regions where wide resection is not possible (mediastinum and retroperitoneum), whereas the tumour is considered to be an atypical lipoma in other locations. Clinically, liposarcomas usually present as a painless soft tissue mass. Only around 10-15% liposarcomas present as a painful soft tissue mass [14]. These can be easily confused with fibromatosis which presents as slow growing single or multiple painful nodular thickenings [24]. A lipoma and a well-differentiated liposarcoma are also quite similar in clinical presentation. MR imaging is an essential tool for detection of liposarcoma as well as for studying its locoregional extension and relations (bone, soft-tissues and neurovascular involvement). MRI can help in differentiating between lipoma, liposarcoma and fibromatosis. Well-differentiated liposarcomas typically demonstrate a largely lipomatous mass, hyperintense on TW1 images, representing over 75% of the lesion in a nodular arrangement separated by thick non-lipomatous septae (>2mm but not exceeding 2cm). The non-lipomatous component shows variable enhancement on fat saturated T1w contrast enhanced images [25,26]. Lipomas also demonstrate abundant adipose tissue homogenously hyperintense on T1w images, similar to well-differentiated liposarcomas. However, lipomas have thin septae (<2mm) and contrast enhancement of lower signal intensity [21]. Fibromatosis on MRI shows nearly the same low-signal intensity as adjacent muscle on T1w and T2w images. Majority of fibromatosis show marked enhancement on gadolinium administration [27,28]. MRI must be performed prior to biopsy or any therapeutic management of a suspected liposarcoma. A well-differentiated liposarcoma appears grossly like a well-circumscribed multi-lobulated mass. Some sections of the tumour reveal mature adipose tissue in abundance that appears identical to a lipoma. However, a well-differentiated liposarcoma can be histologically identified by a typical scattering of lipoblasts with irregularly shaped hyperchromatic nuclei, along with thick fibrovascular septae [16]. Immunohistochemical analysis helps to distinguish a lipoma from a well-differentiated liposarcoma. MDM2 and CDK4 markers are expressed by a well-differentiated liposarcoma [29]. Fibromatosis can be identified based on its characteristic nodular cellular proliferation of plump, spindle shaped cells with intervening collagen with infrequent mitotic figures [30]. Well-differentiated liposarcomas are not known to have malignant potential but local recurrence risk is high [31]. For such tumours of the extremity, the local recurrence rate can be as high as 43% [32]. Such tumours are also reported to have undergone dedifferentiation into a more aggressive form with higher risk of local recurrence and metastasis [9].Prognosis and management of these tumours is related to their anatomical location. Most authors suggest that subcutaneously located tumours can be treated by wide resection, with minimal chances of local recurrence. Radiotherapy is not recommended unless there is gross residual tumour tissue. Chances of recurrence are much higher for tumours in deeper locations. Local recurrence can be treated by re-excision and radiotherapy [32,33,34]. Asymptomatic or mildly symptomatic lipomas of the extremity can be managed conservatively. Troublesome lipomas can be treated by simple excision. The management of fibromatosis can range from conservative management, intralesional steroid injections, collagenase injections, radiotherapy to surgical excision [35,36,37,38,39]. Due to such different lines of management of these pathologies, it is imperative to establish the correct diagnosis before proceeding to treatment. In this case, clinical presentation suggested a diagnosis of plantar fibromatosis, imaging studies suggested the possibility of a lipomatous tumour and histopathological evidence rasied the suspicion of a well differentiated liposarcoma. However, the final diagnosis of plantar fibromatosis was established after correlating the clinical features with a definitve histopathological evaluation following excision of the mass.
conclusions
Although plantar fibromatosis is a commonly encountered disease, it can be mimicked by rare pathologies like lipoma and liposarcoma. Hence, a high index of suspicion is required for their early diagnosis and proper surgical management. Management decisions should be taken after careful correlation between clinical, radiological and histopathological features.
References
1. Ledderhose H. Zur Pathologie der Aponeurose des Fusses und der Hand. Langenbecks Arch Klin Chir. 1897;55:694-712.
2. Cavolo DJ, Sherwood GF. Dupuytrens’s disease of the plantar fascia. J Foot Surg. 1982.21(1):12-15.
3. Weiss SW, Goldblum JR, Enzinger FM. Fibromatoses. In: Weiss SW, Goldblum JR editors. Enzinger and Weiss’ Soft Tissue Tumors. Philadelphia, Pa, USA: Mosby Elsevier;2008. p. 227–228.
4. Lee TH, Wapner KL, Hecht PJ. Plantar fibromatosis. J Bone Joint Surg Am. 1993;75(7):1080–1084.
5. Aviles E, Arlen M, Miller T. Plantar fibromatosis. Surgery. 1971;69(1):117–120.
6. Zgonis T, Jolly GP, Polyzois V, Kanuck DM, Stamatis ED. Plantar fibromatosis. Clin Podiatr Med Surg. 2005;22(1):11-18.
7. Mentzel T, Fletcher CD: Lipomatous tumours of soft tissues: An update. Virchow’s Arch. 1995; 427(4): 353-363.
8. Fletcher CDM, Unni KK, Mertens F. World Health Organization Classification of Tumours. In: Fletcher CDM, Unni KK, Mertens F, editors. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon:IARC Press; 2002. p. 9-18.
9. Weiss SW, Rao VK. Welldifferentiated liposarcoma (atypical lipoma) of deep soft tissue of the extremities, retroperitoneum, and miscellaneous sites. A follow-up study of 92 cases with analysis of the incidence of “Dedifferentiation”. Am J Surg Pathol 1992;16(11):1051-1058.
10. Dei Tos AP. Liposarcoma: New entities and evolving concepts. Ann Diagn Pathol. 2000;4(4):252-266.
11. Fletcher CD. Soft tissue tumours. In: Fletcher CD, editor. Diagnostic histopathology of tumours. 2nd edition. London:Harcourt Publishers Limited; 2000:1473–1540.
12. Kindblom LG, Angervall L, Fassina AS. Atypical lipoma. Acta Pathol Microbiol Immunol Scand [A]. 1982;90(1):27–36.
13. Evans HL, Soule EH, Winkelmann RK. Atypical lipoma, atypical intramuscular lipoma, and well differentiated retroperitoneal liposarcoma: a reappraisal of 30 cases formerly classified as well differentiated liposarcoma. Cancer. 1979;43(2):574–584.
14. Peterson JJ, Kransdorf MJ, Bancroft LW, O’Connor MI. Malignant fatty tumours: classification, clinical course, imaging appearance and treatment. Skeletal Radiol. 2003;32(9):493-503.
15. Munk PL, Lee MJ, Janzen DL, Connell DG, Logan PM, Poon PY, Bainbridge TC. Lipoma and liposarcoma: evaluation using CT and MR imaging. AJR Am J Roentgenol. 1997;169(2):589-594.
16. Enzinger FM, Weiss SW. Liposarcoma. In: Weiss SW, Goldblum JR, Folpe AL, editors. Soft Tissue Tumors. 3rd edition. St. Louis, Mosby, USA: Mosby Elsevier;1995:686-697.
17. Sugar S, Murphy BM. Liposarcoma of the foot; case report. J Mich State Med Soc. 1955;54(4):468–469.
18. Kelly PC, Shramowiat M. Liposarcoma of the foot: a case report. J Foot Surg. 1978;17(1):27–31.
19. Rajasekhar C, Paul AS, Bale RS. Spindle-cell liposarcoma: a rare variant of liposarcoma arising in the foot. Clin Oncol (R Coll Radiol). 2005;17(2):128–129.
20. Matsuo T, Sugita T, Shimose S, Kubo T, Yasunaga Y, Ochi M. Liposarcoma arising in the foot: a case report. Case Rep Med. 2009;2009:630203.
21. Kansdorf MJ, Bancroft LW, Peterson JJ, Murphey MD, Foster WC, Temple HT. Imaging of fatty tumours: distinction of lipoma and well-differentiated liposarcoma. Radiology. 2002;224(1):99-104.
22. Murphey MD, Arcara LK, Fanburg-Smith J. Imaging of musculosketal liposarcoma with radiologic-pathologic correlation. Radiographics 2005;25(5):13711395.
23. Evans H. Liposarcoma: a study of 55 cases with a reassessment of its classification. Am J Surg Pathol. 1979;3(6):507-523.
24. Chokshi FH, Jose J, Clifford PD. Plantar fibromatosis. Am J Orthop. 2009;38(9):475-476.
25. Matsumoto K, Takada M, Okabe H, Ishizawa M. Foci of signal intensities different from fat in well-differentiated liposarcoma and lipoma: correlation between MR and histological findings. J Clin Imaging. 2000;24(1):38-43.
26. Galant J, Martí-Bonmatí L, Sáez F, Soler R, Alcalá-Santaella R, Navarro M. The value of fat-suppressed T2 or STIR sequences in distinguishing lipoma from well-differentiated liposarcoma. Eur Radiol. 2003;13(2):337-343.
27. Walker EA, Petscavage JM, Brian PL, Logle CI, Montini KM, Murphey MD. Imaging features of superficial and deep fibromatoses in the adult population. Sarcoma [Internet]. 2012;2012. Epub 2012 Jun 28, Article ID 215810, 17 pages. Available from Hindawi at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3395298/pdf/SRCM2012-215810.pdf
28. Morrison WB, Schweitzer ME, Wapner KL, Lackman RD. Plantar fibromatosis: a benign aggressive neoplasm with a characteristic appearance on MR images.Radiology. 1994;193(3):841-845.
29. Shimada S, Ishizawa T, Ishizawa K, Matsumura T, Hasegawa T, Hirose T. The value of MDM2 and CDK4 amplification levels using real time polymerase chain reaction for the differential diagnosis of liposarcomas and their histologic mimickers. Hum Pathol. 2006;37(9):1123-1129.
30. Fetsch JF, Laskin WB, Miettinen M. Palmar-plantar fibromatosis in children and preadolescents: a clinicopathologic study of 56 cases with newly recognized demographics and extended follow-up information. Am J Surg Pathol. 2005;29(8):1095-1105.
31. Forus A, Larramendy ML, Meza-Zepeda LA, Bjerkehagen B, Godager LH, Dahlberg AB, Saeter G, Knuutila S, Myklebost O. Dedifferentiation of a welldifferentiated liposarcoma to a highly malignant metastatic osteosarcoma:amplification of 12q14 at all stages and gain of 1q22-q24 associated with metastases. Cancer Genet Cytogenet. 2001;125(2):100-111.
32. Kindblom LG, Angervall L, Svendsen P. Liposarcoma a clinicopathologic, radiographic and prognostic study. Acta Pathol Microbiol Scand Suppl. 1975;(253):1-71.
33. Kang J, Botros M, Goldberg S, Giraud C, Nielsen GP, Chen YL, Raskin K, Schwab J, Yoon SS, Hornicek FJ, Delaney TF. The Use of Radiation Therapy in the Management of Selected Patients with Atypical Lipomas. Sarcoma [Internet]. 2013;2013. Epub on 2013 Jan 15, Article ID 485483, 5 pages. Available from Hindawi at: http://www.hindawi.com/journals/sarcoma/2013/485483/
34. Sommerville SM, Patton JT, Luscombe JC, Mangham DC, Grimer RJ. Clinical outcomes of deep atypical lipomas (well-differentiated lipoma-like liposarcomas) of the extremities. ANZ Journal of Surgery. 2005;75(9):803–806.
35. Sammarco GJ, Mangone PG. Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21(7):563-569.
36. Hammoudeh ZS. Collagenase Clostridium histolyticum injection for plantar fibromatosis (Ledderhose disease). Plast Reconstr Surg. 2014;134(3):497e-498e.
37. Grenfell S, Borg M. Radiotherapy in fascial fibromatosis: a case series, literature review and considerations for treatment of early-stage disease. J Med Imaging Radiat Oncol. 2014;58(5):641-647.
38. McNally EG, Shetty S. Plantar fascia: imaging diagnosis and guided treatment. Semin Musculoskelet Radiol. 2010;14(3):334-343.
39. Aluisio FV, Mair SD, Hall RL. Plantar fibromatosis: treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int. 1996;17(11):672-678.
| How to Cite this article: Bhatnagar N, Lingaiah P, Arora S, Dhal A. Plantar Fibromatosis Masquerading as Liposarcoma : a Case Report and Review of Literature. Journal of Bone and Soft Tissue Tumors May- Aug 2016;2(2):25-29. |

