Langerhans Cell Histiocytosis of the Spine in a Child: A Rare Case and a Diagnostic Dilemma
Original Article | Volume 6 | Issue 3 | JBST September – December 2020 | Page 5-8 | Abigail R Tud, Jose Bayani O Aliling, Carlo Emmanuel J SumpaicoDOI: 10.13107/jbst.2020.v06i03.31
Author: Abigail R Tud[1], Jose Bayani O Aliling[1], Carlo Emmanuel J Sumpaico[1]
[1]Department of Orthopedics, The Medical City, Ortigas Avenue, Pasig City, Metro Manila 1605, Philippines.
Address of Correspondence
Dr. Abigail R Tud,
Unit 5F Tower 1, Sonata Private Residences, Lourdes corner St. Francis Avenues, East Wack Wack, Mandaluyong City, Metro Manila 1505, Philippines.
E-mail address: abitud@gmail.com
Introduction: Langerhans cell histiocytosis (LCH) comprises a rare spectrum of disorders characterized by abnormal proliferation of histiocytes. Lesions may be limited to a single system, or present as disseminated disease, with subsequent worse prognosis. Radiologic findings for spinal LCH are non-specific however and must be carefully differentiated from Pott’s disease (spinal tuberculosis, or [TB]) in endemic countries.
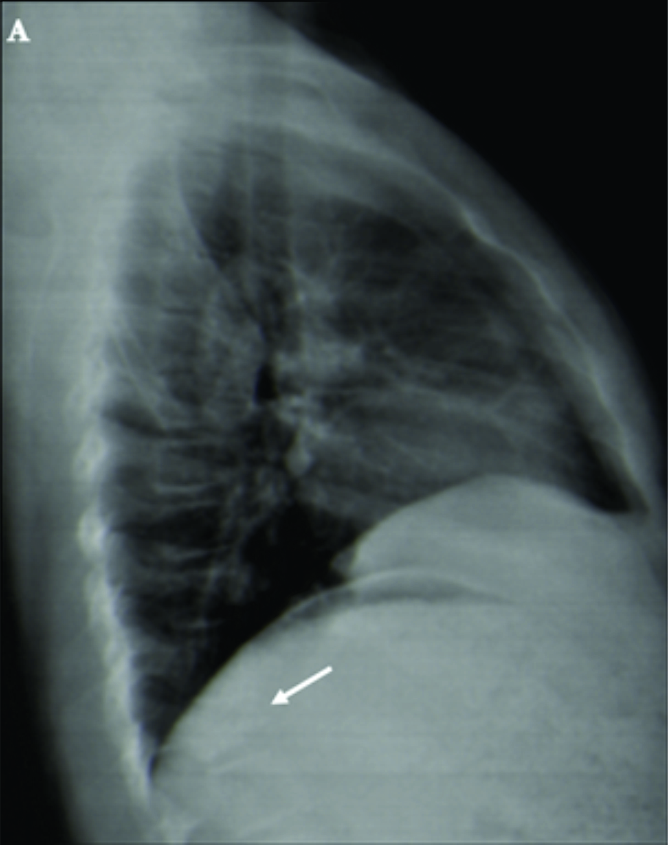
Case Report: An 8-year-old female was brought for consult due to back pain and compression deformity on plain radiographs, unaccompanied by constitutional symptoms. Computed tomography (CT) scan of the thoracic spine was done, which showed osteolysis of the T11 vertebra and paravertebral soft-tissue extension. Findings were deemed suggestive of tuberculous spondylitis, and CT-guided biopsy was performed for confirmation. Acid-fast Bacilli smears as well as Gram stains were negative. While waiting for definitive results, the patient was started on an empiric treatment regimen for TB. Final tissue and fluid cultures were negative for Mycobacterium tuberculosis, as were Gene Xpert and TB polymerase chain reaction studies. Histopathologic analysis showed atypical mononuclear histiocytes surrounded by inflammatory cells, suggestive of LCH. At present, the patient is 2 years post-biopsy, with stable lesions and no evidence of multi-system involvement.
Conclusion: In the setting of a spinal lesion in a child with a benign clinical history and no other pertinent laboratory findings, histopathologic analysis constitutes the gold standard in differentiating non-specific features of LCH from spinal TB. Both conditions necessitate long-term follow-up, due to the risk of progression, deformities, and neurologic sequelae.
Keywords: Langerhans cell histiocytosis, pediatric spine, Pott’s disease, tuberculosis, vertebra plana.
Reference:
1. Imbach P, Kühne T, Arceci RJ. Histiocytoses. In: Pediatric Oncology: A Comprehensive Guide. United States: Springer Science and Business Media; 2011.
2. Lee SW, Kim H, Suh JK, Koh KN, Im HJ, Yoon HM, et al. Long-term clinical outcome of spinal Langerhans cell histiocytosis in children. Int J Hematol 2017;106:441-9.
3. Stålemark H, Laurencikas E, Karis J, Gavhed D, Fadeel B, Henter JI. Incidence of Langerhans cell histiocytosis in children: A population-based study. Pediatr Blood Cancer 2008;51:76-81.
4. Jang KS, Jung YY, Kim SW. Langerhans cell histiocytosis causing cervical myelopathy in a child. J Korean Neurosurg Soc 2010;47:458-60.
5. Peng XS, Pan T, Chen LY, Huang G, Wang J. Langerhans’ cell histiocytosis of the spine in children with soft tissue extension and chemotherapy. Int Orthop 2009;33:731-6.
6. Fellizar KR, Chiong CM. Langerhans cell histiocytosis: An unusual presentation. Philipp J Otolaryngol Head Neck Surg 2008;23:20-4.
7. Garg RK, Somvanshi DS. Spinal tuberculosis: A review. J Spinal Cord Med 2011;34:440-54.
8. Haupt R, Minkov M, Astigarraga I, Schäfer E, Naduri V, Jubran R, et al. Langerhans cell histiocytosis (lch): Guidelines for diagnosis, clinical work-up, and treatment for patients till the age of 18 years. Pediatr Blood Cancer 2013;60:175-84.
9. Huang, WD, Yang XH, Wu ZP, Huang Q, Xiao JR, Yang MS, et al. Langerhans cell histiocytosis of spine: A comparative study of clinical, imaging features, and diagnosis in children, adolescents, and adults. Spine J 2013;3:1-10.
10. Stull MA, Krandsdorf MJ, Devaney KO. Langerhans cell histiocytosis. Radiographics 1992;12:801-25.
11. Department of Health/National TB Control Program Philippine Council for Health Research and Development Foundation for the Advancement of Clinical Epidemiology, Inc. Available from: https://www.philcat.org. [Last accessed on 2018 Sep 29].
12. Xing XY, Yuan HS. Imaging and differential diagnosis of pediatric spinal tuberculosis. Radiol Infect Dis 2015;1:78-82.
13. Rasouli MR, Mirkoohi M, Vaccaro AR, Yarandi KK, Rahimi-Movaghar V. Spinal tuberculosis: Diagnosis and management. Asian Spine J 2012;6:294-308.
14. Gannaban RA, Calimag PP, Zapanta ZS. Langerhans cell histiocystosis presenting as a scalp abscess: A case report. PJSS 2011;66:74-9.
15. Quijano JL, Esguerra AK. Single-system Langerhans cell histiocytosis in a newborn male with positive Tzanck smear. J Philipp Dermatol Soc 2016;25:51-3.
16. Rigor E, Delos Reyes E, Lecciones J, Purugganan H, Fajardo RV. Langerhans’ cell histiocytosis (histiocytosis X) a 12-year retrospective study. Philipp J Pediatr 1993;42:181-9.
17. Villegas MJ, Ke ML. Langerhans’ cell histiocytosis presenting as ulcers. J Philipp Soc Cutan Med 2000;1:90-4.
| How to Cite this article: Tud AR, Aliling JBO, Sumpaico CEJ | Langerhans Cell Histiocytosis of the Spine in a Child: A Rare Case and a Diagnostic Dilemma. | Journal of Bone and Soft Tissue Tumors | September-December 2020; 6(3): 5-8. |


