Limb Salvage With Megaprosthesis In Extremity Osteosarcoma –a Case-based Approach
Volume 2 | Issue 2 | May-Aug 2016 | Page 13-19 | Gurpal Singh, Mark Edward Puhaindran.
Authors: Gurpal Singh[1], Mark Edward Puhaindran[1].
[1]Orthopedic Oncology Services, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai.
Address of Correspondence
Division of Musculoskeletal Oncology, University Orthopaedics, Hand and Reconstructive Microsurgery Cluster, National University Health System, Singapore.
Abstract
Introduction: Musculoskeletal oncology is an evolving field in orthopaedic surgery and surgical management for patients with osteosarcoma has changed fundamentally over the past three decades. Osteosarcoma is a rare tumour, but it is the most common type of primary bone cancer with a biomodal peak. Primary cases tend to occur within the first two decades of life and secondary osteosarcomas affect older patients. Common causes of secondary osteosarcoma include Paget’s disease of bone and radiation exposure. Due to advances in chemotherapeutic regimes, imaging modalities, surgical techniques, material and prosthesis designs, amputation is no longer considered as treatment of choice for most patients. Limb salvage surgery including endoprosthetic reconstructions is also constantly evolving, addressing surgical challenges such as margin control, reconstructive procedures and soft tissue management. In this review, we focus our discussion on the management of patients with osteosarcoma undergoing megaprosthetic reconstruction. Based on three real cases (osteosarcoma of the distal femur, pelvic osteosarcoma involving the hip joint and osteosarcoma of the proximal tibia), this paper aims to highlight surgical challenges that sometimes need to be overcome in this very challenging field.
Keywords: Limb salvage surgery; megaprosthetic reconstruction; osteosarcoma; musculoskeletal oncology.
Introduction
Musculoskeletal oncology is a rapidly evolving field in orthopaedic surgery and surgical management for patients with osteosarcoma has progressed significantly over the past three decades. Due to advances in neoadjuvant treatment, imaging modalities, surgical techniques and material and prosthesis designs, amputation is no longer considered as standard of care in most cases. Literature is currently reporting limb salvage surgeries in 85% to 95% without compromising oncological principles when compared to amputation [1–5]. Main objectives of limb salvage surgery include maximized functional outcome, satisfactory wound coverage for adjuvant therapy and optimized aesthetic outcome without compromising oncologic principles [6]. The reconstructive options for limb salvage surgery can be thought of as biological (autograft, allograft etc.) or endoprosthetic. Sometimes, a combination of both may be necessary. When considering treatment options for patients with osteosarcoma, several factors need to be considered, including the response to neoadjuvant chemotherapy, evidence of periprosthetic fracture, anatomic site, involvement of soft tissue, joint and neurovascular structures as well as the evidence of metastases at diagnosis. Adequate margin control during surgery is crucial. Surgery represents only one component of the multidisciplinary treatment protocol of osteosarcoma patients. Since the 1970s, the role of neoadjuvant therapy has evolved and intense multi-agent chemotherapy has improved the prognosis significantly by eradicating accompanying micrometastases and also reducing the reactive zone around the tumour. The main drawback of chemotherapy prior to surgery includes immunosuppression. Therefore, a multidisciplinary approach between medical oncologists and the surgical team is essential in order to optimise treatment for the patient. After completion of neoadjuvant chemotherapy, re-staging is performed to assess response to chemotherapy and verify resectability and evaluate margins prior to proceeding with definite surgery. Limb salvage surgery for osteosarcoma is typically described as consisting of three parts, starting with en bloc resection of the tumour. Based on the exact location, intra- or extra-articular resection may be considered. In skeletally immature patients, the possibility of physis preservation should be considered. Thereafter, the bone defect is reconstructed. The third part of the surgery consists of soft tissue coverage and functional re-establishment. Treatment protocols for osteosarcoma further include the administration of adjuvant chemotherapy and subsequent long-term surveillance. After limb salvage surgery, overall survival rates of 60% to 70% at 5 years have been reported in literature [1–4, 9, 15]. A recent systematic review and meta-analysis by Stokke et al. evaluating the quality of life among paediatric, adolescent and young adult bone tumour survivors suggested that quality of time improves over time. According to their results, female patients and patients at older age are more likely to have a poor quality of life. Interestingly, there was no difference in outcomes between patients who underwent limb salvage surgery versus amputation for local control [16]. Failure rates in patients undergoing reconstruction with megaprostheses are generally higher compared to patients treated with conventional arthroplasties [7]. However, a direct comparison of study findings is difficult due to different settings and definitions used. Failure rates between 40% to 73% at 5 to 15 years have been reported from factors due to the underlying disease contributing to unfavourable early and late surgical outcome, complications can be specifically related to endoprosthetic reconstruction including aseptic loosening, periprosthetic fracture, infection, implant failure, dissociation of modular components and wear [1, 2, 5, 8, 9]. Implant survival rates for fixed-hinge prostheses have been reported to be approximately 70%, whereas rotating hinge prostheses survival between almost 80 to 100% have been reported [1, 7, 10–13]. A classification system proposed by Henderson et al. for megaprosthesis failure indicates 5 causes of failure, including soft tissue failure (Type 1), aseptic loosening (Type 2), structural fracture (Type 3), infection (Type 4) and local tumour recurrence (Type 5) [14].
Three case examples of patients with osteosarcoma
Case 1 – Osteosarcoma of the distal femur
A 16 year old male patient presented with right knee pain at the lateral aspect of the knee and night pain for about one month. There was no known trauma to the right knee. Clinical findings revealed tenderness over the medial and lateral aspect of the knee and a decreased range of motion 10-110°. Plain radiograph, magnetic resonance imaging, computed tomography and bone scan for local and distal staging were performed, showing an aggressive right distal femoral tumour, with extraosseous soft tissue extension abutting the quadriceps and gastrocnemius muscles, iliotibial band, and medial and lateral gutters of the knee joint (Figure 1a). No fracture or neurovascular involvement was detected. There was no evidence of distant osseous or pulmonary metastases. An open biopsy confirmed the diagnosis of a high-grade conventional osteosarcoma. 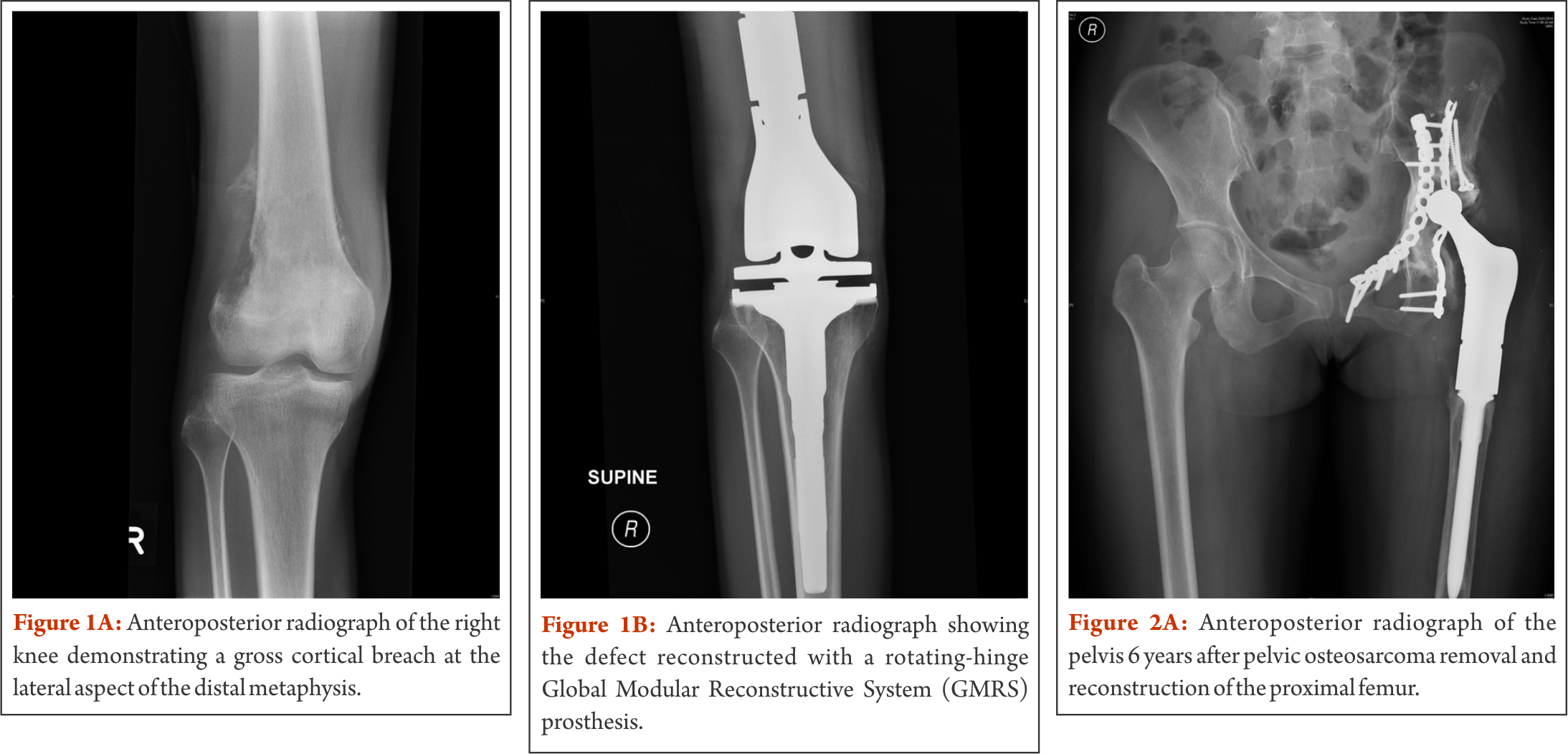
After completion of neoadjuvant chemotherapy, the patient developed an extensive local fungal infection on the lateral aspect of the thigh, surrounding the biopsy incision site. Systemic antifungal therapy was given for two weeks, directed by a dermatologist and surgery was delayed by two weeks. Given the small window of opportunity between neoadjuvant and adjuvant chemotherapy and to minimise further delay in treatment, the surgical team in the outlined case decided to proceed with tumour resection. In view of the recent tinea corporis with lesions on the lateral aspect of the right thigh, the decision was made to proceed with an anteromedial approach with the excision of the biopsy tract laterally. Local tumour recurrence as a result of spread of malignant cells during biopsy has been reported [17, 18]. Consequently, the biopsy tract is considered as contaminated and conventionally excised during tumour removal. However, more recent studies have shown preliminary evidence for the safety of limb salvage surgery without biopsy tract excision following a diagnostic core needle biopsy and fine-needle aspiration, respectively [19, 20]. In the outlined case, a medial dissection via interval between vastus medialis and rectus femoris was performed for en bloc resection of the tumour. Femoral vessels were identified and traced into the popliteal fossa via adductor canal. The femur osteotomy was made at pre-templated 150 mm from the joint line. The sciatic and peroneal nerve were identified and preserved. Histopathological analysis of frozen sections and tumour specimen showed negative margins. After change of instruments, distal femur reconstruction was continued. Femur and tibia were prepared and a rotating-hinge Global Modular Reconstructive System (GMRS) (Stryker Inc, Rutherford, NJ, USA) knee prosthesis was used for reconstruction (Figure 1b). The vastus medialis was mobilised and brought down to cover the defect medially. The extensor mechanism was reconstructed over the prosthesis. No post-operative complications occurred, all wounds healed satisfactorily. Six months after surgery, the patient is walking without any support. This case highlights the necessity of non-conventional surgical approaches when necessary. Although the main tumour burden was on the lateral aspect of the knee joint, given the location of the previous treated fungal infection, the decision for a medial approach was made. Extra- versus intraarticular resection needs to be discussed in the appropriate context. Preliminary evidence is hinting towards an overestimation of neoplasm seeding in the biopsy tract, especially when the biopsy is performed by the operating surgeon himself. The point to emphasize in this case is the close communication between medical oncologist and the surgeon and balancing the risks of delaying adjuvant chemotherapy versus an “unconventional” surgical approach. This patient underwent an intraarticular resection of the distal femur. In cases where the knee joint is found to be contaminated or being directly invaded by the tumour, an extraarticular resection of the entire joint with en-bloc removal is recommended. Usually, this approach is associated with poorer functional results.
Case 2 – Pelvic osteosarcoma involving the hip joint
A 24 year old female patient presented with a left neck of femur fracture with underlying osteosarcoma. Prognostic and treatment implications of pathological fractures at presentation have been widely debated. In the past, pathological fractures have been considered as indication for amputation due to the risks of local recurrence from contamination caused by the fracture hematoma. However, a recent systematic review and meta-analysis by Salunke et al. is demonstrating similar rates of local recurrence in patients with limb salvage surgeries compared to amputation, provided carefully selection of patients has been performed [21]. Our own 18-year experience of high-grade osteosarcoma with a pathological fracture at initial presentation showed no differences in the survival and recurrence rates of patients with pathological fractures compared to those with no fractures. Moreover, we did not see any difference in survival between amputated and salvaged patients with fractures, provided margin control attempts are aggressive (unpublished data). In the outlined case, the patient was treated according to protocol with neoadjuvant chemotherapy. Given the complexity of the case, but still aiming for limb salvage, the decision was made for using endoprosthetic and biologic reconstructive options, namely the combination of a hemipelvectomy with an extra-articular proximal femur resection followed by proximal femur replacement and acetabular column plating/deep frozen bone (Fig. 2a). Biologic reconstruction options such as allografts, autografts and re-implantation of sterilized tumour bone replace the defect with a biologic construct, providing the theoretical advantage of incorporation of the biological graft. However, retrieval studies have shown that grafts become necrotic and may act as a spacer rather than a stable replacement. Typical failures include graft-fracture, non-union between the graft and host-bone and increased infection-rates. Drawbacks also include the dependence of graft incorporation for rehabilitation. A reliable tissue bank and associated logistics are sine qua non, and harvesting the autograft or preparing the allograft and subsequently increasing surgical time need to be taken into account. Since a long-term study showed that less than 50% of allografts lasted less than 10 years [22], this technique is mostly preserved for special occasions only, such as osteosarcomas in skeletally immature patients without involving the growth plates. Combined usage of endoprosthetic and biologic reconstruction is described by the allograft prosthetic composite. The concept behind includes restoration of the bone stock by allograft and using endoprosthetic components to restore articulating surfaces, theoretically offering a higher durability in the long-term when compared to pure biologic reconstruction. In the outlined case, the patient’s own pre-treated tumour bone was used for part of the recontruction. Sterilization of the bone can be performed in various ways including pasteurizing, autoclaving, radiotherapy, and freezing. Similarly to the use of allografts, non-union, infection and fracture belong to the main complications in biologic reconstruction with autografts. As described in the outlined case, liquid nitrogen was used for pre-treatment of the bone. Cryosurgery in combination with autograft-prosthesis composites shows promising results with excellent functional outcomes, low complication rates and improved union rates, especially when used with the pedicle-freezing technique [23–25]. After completion of adjuvant chemotherapy and being in remission, the patient in the outlined case developed a hematogenous methicillin susceptible staphylocococcus aureus (MSSA) infection of the endoprosthesis six years postoperatively. Infection is still the most common complication in megaprosthetic reconstruction and in general, it is more likely to happen when adequate wound coverage is missing. In primary megaprosthesis infection rates between 2% to 20% have been reported, with the numbers increasing to more than 40% in revision cases [1, 2, 5, 10, 14, 26–31]. The classic approach in periprosthetic infection is a two-stage exchange revision surgery, including the removal of original endoprosthetic components, thorough debridement, administration of intravenous antibiotics, and implantation of a spacer followed by the re-implantation of implants. In the outlined case, this approach was not practical. A consensus with the multidisciplinary musculoskeletal oncology team and the patient was made for management with ultrasound-guided drainage of the left hip joint and suppressive antibiotics with follow-ups by our colleagues for infectious disease. The patient was discharged with peripherally inserted central catheter line in situ. She continued to develop a collection in the left hip and anterior thigh. A formal arthrotomy with extensive debridement and removal of all necrotic tissue was performed. A large bore chest drain was left in situ, exited through quadriceps anteriorly, plus two additional drains subcutaneously. An urostomy pouch was applied and the patient was kept on long term drainage, allowing the sinus track to the left lateral thigh to mature. In the following, kept with suppressive antibiotics (ciprofloxacin and rifampicin), the patient was under close follow-up with a regular change of the urostomy bag. Erythema and tenderness regressed and drainage successively decreased (Figure 2b). The chest drain was removed two months after surgery. On examination, 29 months after debridement the left thigh is non-tender and showed no erythema. Scars to the left tight (sinus track) are well healed and she had no fever, chills or rigor and denied any pain. She is walking with a slight limp and was returned to work recently. She remains on long-term suppressive antibiotics as guided by the infectious disease physician. This case highlights how limb salvage surgery has pushed the boundaries over the last decades. Combining different reconstructive options may be considered for complex cases. This case also illustrates the option of a relatively conservative management strategy for periprosthetic infection in a compliant patient, achieving a satisfactory result. 
Case 3 – Osteosarcoma of the proximal tibia
A 16 year old female patient was diagnosed with non metastatic osteosarcoma of the left proximal tibia (stage IIb). She underwent left tibial osteosarcoma resection, reconstruction with megaprosthesis, extensor mechanism reconstruction, medial gastrocnemius flap and split skin graft (Figure 3a and 3b). Proximal tibia resection presents unique local anatomical features which need to be addressed during limb salvage surgery. Neurovascular structures in the popliteal fossa as well as the peroneal nerve between the biceps femoris and the lateral head of the gastrocnemius muscle need to be preserved as much as possible. Displacement of these structures due to a large tumour mass are likely, therefore careful preparation in this area is required. In most cases, biological borders such as perivascular fat or the popliteus muscle are separating the tumour from the neurovascular bundle. Intraoperatively, overstretching these structures due to overdistraction of the femur and tibia (after resecting the tumour) needs to be avoided in order to prevent neuropraxia and endothelial injury. Involvement of tissue adjacent to the tibiofibular joint is usually of concern and this joint is typically included in the resection. Once the patellar tendon has been divided, reconstruction of the extensor mechanism is obligatory. Various techniques to attach the tendon to the endoprostetic implant have been described in a systematic review by Ek et al. including direct fixation using screw/washer or sutures, synthetic soft tissue augments such as tubes, sutures, cerclage wires and non-absorbable tapes and biological augmentation such as graft from the biceps or satorius tendons or gastrocnemius flaps with or without synthetic materials [32]. The authors report a trend towards improved outcomes with biologic reconstructive options. However, there is no clear evidence for a single technique. Extensor lag is of major concern in all surgeries requiring reconstruction of the extensor mechanism. Therefore, postoperative management in the outlined case included immobilization with a long-leg cast and a long-leg brace respectively for six weeks to allow healing. Obtaining full extension and allowing the extensor mechanism to heal was given priority compared to knee flexion in view of its impact on ambulation and there was a strong emphasis on extensor mechanism strengthening during rehabilitation. The close proximity of the proximal tibia to the skin makes the wound more susceptible to infectious complications. Keeping thick flaps during preparation at the beginning of the surgery minimize necrosis of the skin. Typically, a primary medial gastrocnemius flap is used to improve wound coverage with the advantage of offering a larger muscular material and also bypassing a longer distance when compared to the lateral gastrocnemius [33, 34]. This technique has been first described by Dubousset et al. [35]. Skin grafting provides an additional supportive procedure while relieving tension during skin closure and therefore preventing skin flap necrosis. Currently, split-thickness skin graft is considered as gold standard in any major skin loss. Typically, the graft is meshed in order for expansion while keeping the morbidity to the donor side as low as possible. Postoperative management in patients with skin grafts includes a close observation of the donor side for scarring, pain and signs suggestive of infection. This case illustrates a conventional proximal tibia resection, highlighting surgical considerations with regards to anatomical characteristics and postoperative management.
conclusions
Medical management, surgical techniques and prosthetic design have improved significantly during the last three decades. Amputation is no longer considered as standard of care in patients with osteosarcoma in most cases. However, limb salvage with megaprosthesis remains challenging. Complication rates are high, with infection occurring most commonly. A good interaction within a multidisciplinary team in a preferably high-volume centre is required for optimal management. Given the unique features of these patients, “unconventional” approaches and combinations of reconstructive options may be considered sometimes, provided oncologic principles are not compromised.
References
1.Pala E, Trovarelli G, Calabrò T, Angelini A, Abati CN, Ruggieri P. Survival of modern knee tumor megaprostheses: failures, functional results, and a comparative statistical analysis. Clin Orthop Relat Res 2015;473:891–9.
2.Zeegen EN, Aponte-Tinao LA, Hornicek FJ, Gebhardt MC, Mankin HJ. Survivorship analysis of 141 modular metallic endoprostheses at early followup. Clin Orthop Relat Res 2004:239–50.
3.Bacci G, Ferrari S, Bertoni F, Ruggieri P, Picci P, Longhi A, et al. Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the istituto ortopedico rizzoli according to the istituto ortopedico rizzoli/osteosarcoma-2 protocol: an updated report. J Clin Oncol 2000;18:4016–27.
4.Bacci G, Picci P, Ferrari S, Ruggieri P, Casadei R, Tienghi A, et al. Primary chemotherapy and delayed surgery for nonmetastatic osteosarcoma of the extremities. Results in 164 patients preoperatively treated with high doses of methotrexate followed by cisplatin and doxorubicin. Cancer 1993;72:3227–38.
5.Gosheger G, Gebert C, Ahrens H, Streitbuerger A, Winkelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res 2006;450:164–71.
6.Heller L, Kronowitz SJ. Lower extremity reconstruction. J Surg Oncol 2006;94:479–89. doi:10.1002/jso.20485.
7.Heisel C, Kinkel S, Bernd L, Ewerbeck V. Megaprostheses for the treatment of malignant bone tumours of the lower limbs. Int Orthop 2006;30:452–7.
8.Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol 2013;107:335–42.
9.Orlic D, Smerdelj M, Kolundzic R, Bergovec M. Lower limb salvage surgery: modular endoprosthesis in bone tumour treatment. Int Orthop 2006;30:458–64.
10.Ahlmann ER, Menendez LR, Kermani C, Gotha H. Survivorship and clinical outcome of modular endoprosthetic reconstruction for neoplastic disease of the lower limb. J Bone Joint Surg Br 2006;88:790–5.
11.Bhangu AA, Kramer MJ, Grimer RJ, O’Donnell RJ. Early distal femoral endoprosthetic survival: cemented stems versus the Compress implant. Int Orthop 2006;30:465–72.
12.Myers GJC, Abudu AT, Carter SR, Tillman RM, Grimer RJ. Endoprosthetic replacement of the distal femur for bone tumours: long-term results. J Bone Joint Surg Br 2007;89:521–6. doi:10.1302/0301-620X.89B4.18631.
13.Ruggieri P, Mavrogenis AF, Pala E, Abdel-Mota’al M, Mercuri M. Long term results of fixed-hinge megaprostheses in limb salvage for malignancy. Knee 2012;19:543–9.
14.Henderson ER, Groundland JS, Pala E, Dennis JA, Wooten R, Cheong D, et al. Failure mode classification for tumor endoprostheses: retrospective review of five institutions and a literature review. J Bone Joint Surg Am 2011;93:418–29.
15.Eckardt JJ, Eilber FR, Dorey FJ, Mirra JM. The UCLA experience in limb salvage surgery for malignant tumors. Orthopedics 1985;8:612–21.
16.Stokke J, Sung L, Gupta A, Lindberg A, Rosenberg AR. Systematic review and meta-analysis of objective and subjective quality of life among pediatric, adolescent, and young adult bone tumor survivors. Pediatr Blood Cancer 2015;62:1616–29.
17.Schwartz HS, Spengler DM. Needle tract recurrences after closed biopsy for sarcoma: three cases and review of the literature. Ann Surg Oncol 1997;4:228–36.
18.Davies NM, Livesley PJ, Cannon SR. Recurrence of an osteosarcoma in a needle biopsy track. J Bone Joint Surg Br 1993;75:977–8.
19.Saghieh S, Masrouha KZ, Musallam KM, Mahfouz R, Abboud M, Khoury NJ, Haidar R. The risk of local recurrence along the core-needle biopsy tract in patients with bone sarcomas. Iowa Orthop J 2010;30:80–3.
20.Kaffenberger BH, Wakely PE, Mayerson JL. Local recurrence rate of fine-needle aspiration biopsy in primary high-grade sarcomas. J Surg Oncol 2010;101:618–21.
21.Salunke AA, Chen Y, Tan JH, Chen X, Khin LW, Puhaindran ME. Does a pathological fracture affect the prognosis in patients with osteosarcoma of the extremities?: A systematic review and meta-analysis. Bone Joint J 2014;96-B:1396–403. doi:10.1302/0301-620X.96B10.34370.
22.Brigman BE, Hornicek FJ, Gebhardt MC, Mankin HJ. Allografts about the Knee in Young Patients with High-Grade Sarcoma. Clin Orthop Relat Res 2004:232–9.
23.Subhadrabandhu S, Takeuchi A, Yamamoto N, Shirai T, Nishida H, Hayashi K, et al. Frozen Autograft-Prosthesis Composite Reconstruction in Malignant Bone Tumors. Orthopedics 2015;38:e911-8.
24.Jeon D, Kim MS, Cho WH, Song WS, Lee S. Pasteurized autograft-prosthesis composite for distal femoral osteosarcoma. J Orthop Sci 2007;12:542–9. doi:10.1007/s00776-007-1173-7.
25.Jeon D, Kim MS, Cho WH, Song WS, Lee S. Pasteurized autograft-prosthesis composite for reconstruction of proximal tibia in 13 sarcoma patients. J Surg Oncol 2007;96:590–7.
26.Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, Gosheger G. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg 2006;126:289–96.
27.Lee SH, Oh JH, Lee KS, Yoo KH, Kim HS. Infection after prosthetic reconstruction in limb salvage surgery. Int Orthop 2002;26:179–84. doi:10.1007/s00264-001-0328-y.
28.Unwin PS, Cannon SR, Grimer RJ, Kemp HB, Sneath RS, Walker PS. Aseptic loosening in cemented custom-made prosthetic replacements for bone tumours of the lower limb. J Bone Joint Surg Br 1996;78:5–13.
29.Grimer RJ, Belthur M, Chandrasekar C, Carter SR, Tillman RM. Two-stage revision for infected endoprostheses used in tumor surgery. Clin Orthop Relat Res 2002:193–203.
30.Horowitz SM, Lane JM, Otis JC, Healey JH. Prosthetic arthroplasty of the knee after resection of a sarcoma in the proximal end of the tibia. A report of sixteen cases. J Bone Joint Surg Am 1991;73:286–93.
31.Jeys LM, Grimer RJ, Carter SR, Tillman RM. Periprosthetic infection in patients treated for an orthopaedic oncological condition. J Bone Joint Surg Am 2005;87:842–9. doi:10.2106/JBJS.C.01222.
32.Ek EW, Rozen WM, Ek ET, Rudiger HA. Surgical options for reconstruction of the extensor mechanism of the knee after limb-sparing sarcoma surgery: an evidence-based review. Arch Orthop Trauma Surg 2011;131:487–95.
33.McCraw JB, Fishman JH, Sharzer LA. The versatile gastrocnemius myocutaneous flap. Plast Reconstr Surg 1978;62:15–23.
34.Meller I, Ariche A, Sagi A. The role of the gastrocnemius muscle flap in limb-sparing surgery for bone sarcomas of the distal femur: a proposed classification of muscle transfers. Plast Reconstr Surg 1997;99:751–6.
35.Dubousset J, Missenard G, Genin J. Traitement chirurgical conservateur des sarcomes ostéogéniques des membres. Techniques et résultats fonctionnels. Rev Chir Orthop Reparatrice Appar Mot 1985;71:435–50.
| How to Cite this article: Singh G, Puhaindran ME. Limb Salvage With Megaprosthesis In Extremity Osteosarcoma –a Case-based Approach. Journal of Bone and Soft Tissue Tumors May- Aug 2016;2(2):13-19 . |