Re implantation of Sterilised tumour bone by Extra Corporeal Radiotherapy
Vol 1 | Issue 1 | May – August 2015 | page:37-39 | Subin Sugath[1*].
Author: Subin Sugath[1*].
[1]Department of Aster Orthopaedics, Aster DM Healthcare Pvt Ltd., Kochi 682 027, Kerala, India.
Address of Correspondence
Dr. Subin Sugath MS Orth.
Department of Ortho Oncology. Aster DM Healthcare Pvt Ltd. Kuttisahib Road, Near Kothad Bridge, South Chittoor PO, Cheranallor, Kochi 682 027, Kerala, India.
Email: drsubin.sugath@dmhealthcare.com
Abstract
With the use of potent chemotherapeutic drugs, newer imaging modalities and improved surgical techniques limb preserving surgeries for malignant bone tumours have become the norm. Endoprosthesis still remains the commonest method of reconstruction after tumour resection. But when one is able to an oncologically safe intercalary resection for malignant bone tumours one method of reconstruction is reimplanting the resected tumour bone after sterilisation. Radiation given outside the body to sterilise the tumour bone is called Extra Corporeal Radiotherapy (ECRT). After resection the bone is cleaned of all its soft tissue and marrow contents and sent in a plastic container to the Radiotherapy department where it is subjected to 50 Gy of radiation which kills all cells including the tumour cells. The bone is brought back to the theatre and reimplanted after augmenting it with either bone cement or fibular grafts and stabilised by appropriate fixation devices. The advantage of reimplanting the same bone is that you get an exact match to the resected bone which is tumour free. Post operatively the joint is mobilised immediately and weight bearing started as appropriate to the fixation used. The diaphyseal end takes more time to unite than the metaphyseal end. In our series of 16 patients who had undergone ECRT and reimplantation for malignant bone tumours of the extremity and had completed two year follow up, the metaphyseal end took an average of 6.2 months (4 – 12 months) for union while the diaphyseal end united in 10.6 months (5 – 15 months). If the tumour has caused extensive destruction of the bone or has a pathological fracture, it may be mechanically not sound to reimplant it after ECRT. ECRT is an oncologically safe and mechanically stable procedure in biologically reconstructing bony defects after tumour resection.
Keywords: Extra Corporeal Radiotherapy, Bone tumour, intercalary resection.
Introduction
With the use of potent chemotherapeutic drugs, newer imaging modalities and improved surgical techniques limb preserving surgeries for malignant bone tumours have become the norm. Endoprosthetic replacement is the most commonest method used to bridge the bone defect after tumour resection [1]. Such resection commonly involve resection of the growth physis across the joint leading to limb length disparity as the child grows. To overcome this, one will have to use a growing prosthesis which can be lengthened post operatively either by invasive or non invasive techniques to compensate for the growth of the normal limb [2] These implants are expensive and are not affordable to majority of patients who undergo limb salvage surgery in our country
At times, especially in young children where the open physis can be taken as a wide margin the tumour can be resected with wide margins sparing the joint ant the physis. The bone defects after these resection can be bridged by intercalary implants or size matched allografts if one has access to good tissue bank. Biological method of reconstruction has the advantage that once it incorporates with the host bone it is a life long procedure and is not associated with the complications of using a prosthesis [3,4]. Alternative technique of biological reconstruction if one does not have access to a tissue bank would be to use a vacularised or non vascularised autograft like fibula. But at times it would be impossible to harvest enough autografts to bridge large bony defects [5]. Sterilising and reimplanting the resected tumour bone is a viable option in these situations.
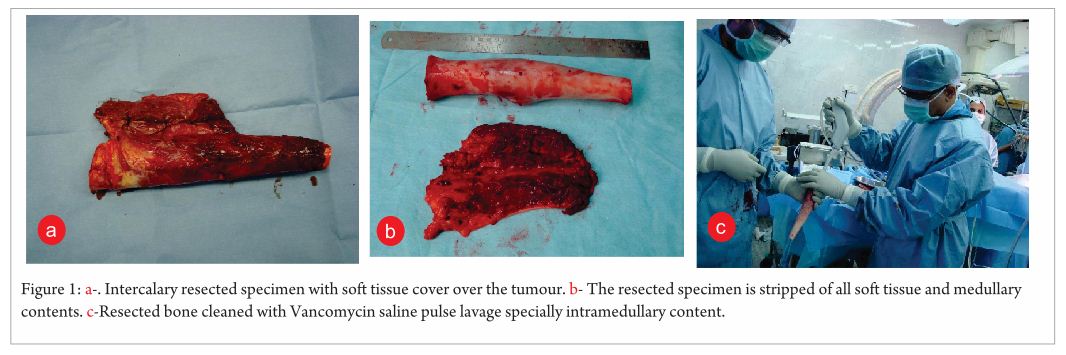
The advantage of reimplanting the same bone is that you get an exact match to the resected bone which is tumour free. The different methods used to sterilise tumour bone are autoclaving, pasteurisation, liquid nitrogen and radiotherapy [6]. Autoclaving involves sterilising the bone at 1210 C for 20 minutes which kills all tumour cells. But it has got the disadvantage that it reduces the bone strength as well as destroys the Bone Morphogenic Protein (BMP) [7]. Sterilising the specimen in a water bath at 650 C for 30 minutes is called pasteurisation. It has the advantage it retains the bone strength and BMP but has the practical difficulty of maintain the sterility during the procedure [6,8]. The most common method of sterilisation technique used is radiotherapy. 50 Gy of single shot high dose radiotherapy is used to sterilise the tumor bone. The procedure of giving radiotherapy outside the human body is called Extra Corporeal Radiotherapy (ECRT). The dose of radiotherapy given is so high that it destroys all cells including the tumour cells which necessitates this dose to be given outside the human body. The mechanical strength of the bone is least affected by this procedure and there are enough publications in literature which show this to be an oncological safe procedure in sterilising tumour bone. 50 Gy of radiotherapy is sufficient in attain tumour kill [9,10,11] and any higher dose of radiation decreases the mechanical strength and revascularisation and delays graft union and incorporation. The resection is made as per the pre operative imagings (Fig 1a). Marrow curettings from both the proximal and distal cut ends are send for frozen study to ensure adequacy of tumour clearance. Intercalary resected specimen with soft tissue cover over the tumour. Now the bone is completely stripped of all its soft tissue, periosteum and medullary contents (Fig 1b). The soft tissue removed is oriented with suture tags so that adequacy of tumour clearance can be assessed by histopathological examination. The bone is thoroughly washed with Vacomycin saline using a pulse lavage (Fig 1c).
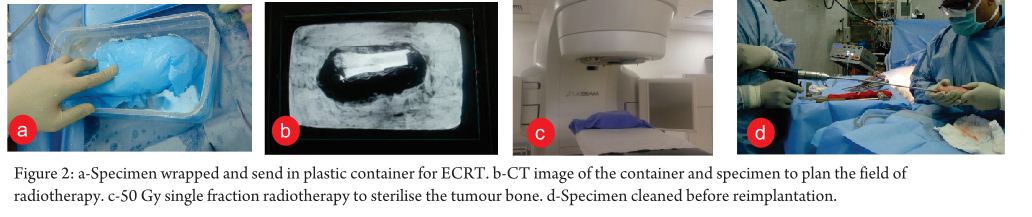
 The vancomycin which gets absorbed by the graft is eluded over a period of time when it is reimplanted. The cleaned specimen is put in a plastic container and sent for radiotherapy (Fig 2a).
The vancomycin which gets absorbed by the graft is eluded over a period of time when it is reimplanted. The cleaned specimen is put in a plastic container and sent for radiotherapy (Fig 2a).
Care is taken to eliminate free space in the container with saline and cotton pads to eliminate air as air causes dispersion of radiation. Specimen is taken to the radiotherapy department and as described earlier 50 Gy of single shot radiotherapy is given to the specimen after planning CT scan (Fig 2b,2c). This procedure takes between 30 – 90 minutes depending on the radiation machine used. The specimen is then brought back to the theatre and cleaned and washed with Vancomycin saline (Fig 2d).
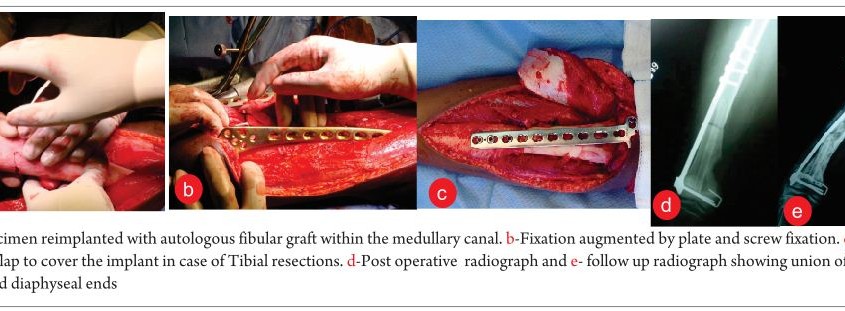
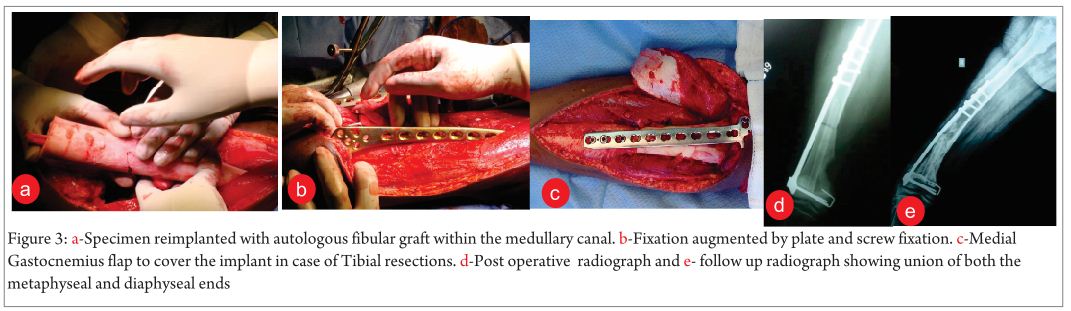
The medullary canal of the sterilised bone can either be filled with bone cement or fibular graft to add on to the osteoconductive property (Fig 3a). The graft is re-implanted and stabilised by appropriate plate and screw fixation (Fig 3b). Care must be taken to put only minimal screws in the re-implanted graft during fixation. In case of tibial lesions an additional medial gastrocnemius flap may be needed for covering the sub cutaneous implants (Fig 3c). Post operatively the joint is mobilised immediately and weight bearing started as appropriate to the the fixation used. Patients are followed up at the routine frequency practised for malignant bone tumours. Radiological, oncological and functional assessment are done at each visit. The diaphyseal end takes more time to unite than the metaphyseal end. In our series of 16 patients who had undergone ECRT and reimplantation for malignant bone tumours of the extremity and had completed two year follow up, the metaphyseal end took an average of 6.2 months (4 – 12 months) for union while the diaphyseal end united in 10.6 months ( 5 – 15 months) (Fig 3c, 3d).
There were two cases of non union at the diaphyseal end for which subsequent bone grafting was required to attain union.
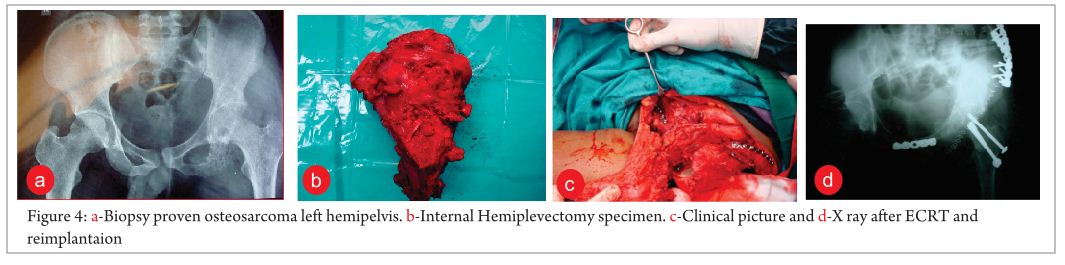
ECRT can also be used in reconstruction of bony defects after Internal Hemipelvectomy for malignant tumours of the pelvis. Here like in the long bones the tumour can be resected with margins as per the pre chemotherapy imagings and reimplanted after ECRT and fixed with appropriate plate and screw fixation (Fig 4a-d).
ECRT and reimplantation is an inexpensive method of reconstruction which can be carried out even in hospitals without radiation facility. The specimen after resection can be transported to the nearby centre having radiation facility where ECRT can be done and brought back and reimplanted. This method eliminates the need to have a tissue bank in hospital for doing biological reconstruction and also is not associated with the complications of using massive allografts. This technique also has the advantage that it provides an exact size matched graft for reconstruction.
If the tumour has caused extensive destruction of the bone or has a pathological fracture, it may be mechanically not sound to reimplant it after ECRT and alternative methods of reconstruction like intercalary implants or allografts would be ideal. Graft fracture is one complication that can occur in this procedure. This can be reduced by using appropriate fixation devices which bridge the whole length of the graft and also augmenting the graft with bone cement or fibular graft.
ECRT is an oncologically safe and mechanically stable procedure in biologically reconstructing bony defects after tumour resection. But the success of the procedure depends on appropriate patient selection, meticulous preoperative planning, implementing these plans intra operatively and the infrastructure backup to support it.
References
1. Gosheger, G.; Gebert, C.; Ahrens, H.; Streitbuerger, A.; Winkelmann, W.; Hardes, J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin. Orthop. Relat. Res. 2006, 450, 164–171.
2. Kotz, R.I.; Windhager, R.; Dominkus, M.; Robioneck, B.; Muller-Daniels, H. A self-extending paediatric leg implant. Nature 2000, 406, 143–144.
3. Tsuchiya H, Tomita K, Minematsu K, et al. Limb salvage using distraction osteogenesis: a classification of the technique: J Bone Joint Surg [Br] 1997;79-B:403–11.
4. Plotz W, Rechl H, Burgkart R, et al. Limb salvage with tumor endoprostheses for malignant tumors of the knee: Clin Orthop 2002;405:207–15.
5. Ceruso M, Falcone C, Innocenti M, Delcroix L et al. Reconstruction with a free vascularized fibula graft associated to bone allograft after resection of malignant bone tumor of limbs. Handchir. Mikrochir. Plast. Chir. 2001, 33, 277–282.
6. Singh VA, Nagalingam J, Saad M, Pailoor J: Which is the best method of sterilization of tumour bone for reimplantation? A biomechanical and histopathological study : Biomed Engineering OnLine 2010, 9:48.
7.Kok Long Pan, Wai Hoong Chan, Gek Bee Ong, Shanmugam Premsenthil et al. Limb salvage in osteosarcoma using autoclaved tumor-bearing bone: Pan et al. World Journal of Surgical Oncology 2012,10:105
8.Jyoti Kode, Prasad Taur, Ashish Gulia, Nirmala Jambhekar, Manish Agarwal, and Ajay Puri. Pasteurization of bone for tumour eradication prior to reimplantation – An in vitro & pre-clinical efficacy study; Indian J Med Res. 2014 Apr; 139(4): 585–597.
9.Mondelaers W, Van Laere K, Uyttendaele D. Treatment of primary tumours ofbone and cartilage by extracorporeal irradiation with a low energy high power electron linac; Nuclear Instruments Methods in Physics Res 1993;70-B:898-900.
10.Hong A, Stevens G, Stalley P, et al. Extracorporeal irradiation for malignant bone tumours. Int J Radiat Oncol Biol Phys 2001;50:441-7
11.Sharma D N, Rastogi S, Bakhshi S, Rath G K, Julka P K, Laviraj M A, Khan S A, Kumar A. Role of extracorporeal irradiation in malignant bone tumors. Indian J Cancer 2013;50:306-9.
| How to Cite this article: Sugath S. Re implantation of Sterilised tumour bone by Extra Corporeal Radiotherapy. Journal of Bone and Soft Tissue Tumors May-Aug 2015; 1(1):37-39. |
 Dr.Subin Sugath |
