Intractable Knee pain….it could be Glomus!
Vol 1 | Issue 1 | May – August 2015 | page:48-50 | Umesh M Kulkarni[1], Vijay Zavar[2], Sudhir Sankalecha[3], Ameya Kulkarni[1].
Author: Umesh M Kulkarni[1], Vijay Zavar[2], Sudhir Sankalecha[3], Ameya Kulkarni[1].
[1]Sanjivan Hospital, India Security Press Hospital, Nashik, Maharashtra, India.
[2]Skin Diseases Center, Nashik, Maharashtra, India.
[3]Sankalecha Labs, Nashik, Maharashtra, India.
Address of Correspondence
Dr. Umesh M Kulkarni
Sanjivan Hospital, India Security Press Hospital, Nashik, Maharashtra, India.
Email : umesh_kulkarni76@yahoo.com
Abstract
Introduction: Glomus tumors are areteriovenous anastomoses mostly found on flexor surfaces of fingers and nail beds. Occurrences in lower extremity is rarity and requires high index of suspicion.
Case Report: Thirty eight year old housewife presented with severe knee pain and swelling on the medial side of the knee since last two years. She had taken multiple opinions and was on analgesics and anti inflammatory medications for an extended duration. On examination an ill defined tender nodule was palpable on superolateral aspect of patella. MRI showed hypointense nodule with uniform contrast uptake. Excision biopsy was done to remove the lesion in total. Patient has complete relief of symptoms. Histopathology confirmed the diagnosis of glomus tumor
Conclusion: Glomus tumors can rarely occur in unusual locations. Clinical presentation and MRI help to narrow down the diagnosis. Excision leads to complete relief of symptoms.
Keywords: Glomus tumor, Knee, excision biopsy.
Introduction
The glomus body is a specialised form of arteriovenous anastomosis localised in the dermal soft tissue and acts as a thermoregulator. A glomus tumour (glomangioma, tumors of Popoff, or Barré-Masson syndrome) is a benign mesenchymal neoplasm composed of cells which resemble the modified smooth muscle cells of the normal glomus body (glomocytes) [1]. Extra-digital location of glomus tumour is uncommon [2]. Considering the rarity of this site, we present this case of Glomus tumour (GT) of the knee.
Case Report
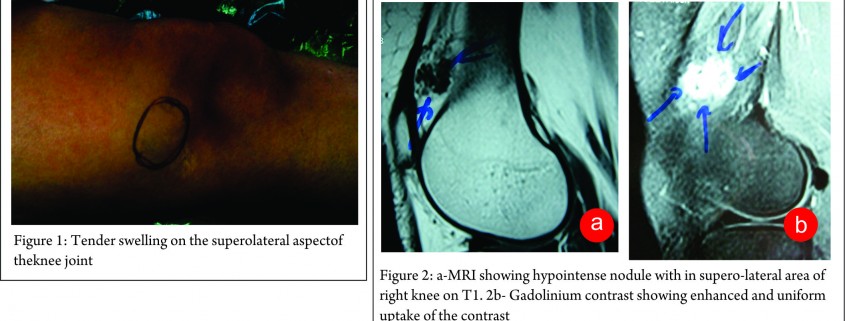
A 38-yr-old housewife presented with severe right knee pains, supero-laterally to the patella, progressive since 2 years. Even the gentle touch would result in disproportionate shooting or stabbing type of pains, sometimes associated with paraesthesia. At times, the touch of clothing was unbearable. There was no seasonal exacerbation of the pains, which increased on extreme flexion of the knee or sitting cross-legged, compromising her daily work. She had abnormal apprehensive behaviour towards any person or object near her knee. There was no history of trauma or any inflammatory episode of the knee. She had received a number of analgesics, anti-inflammatory and anti-psychotic agents without much relief. She was even advised a psychiatric consultation prior to coming to us. On examination, an ill-defined soft nodule was palpable at the point of maximum tenderness only on extreme flexion of the knee (Fig.1). It was exquisitely tender on deep palpation. Movements of knee were painful in terminal flexion. There was no increase in local temperature. Swelling was mobile in the transverse direction, indicating adherence to deeper fibrous layers.
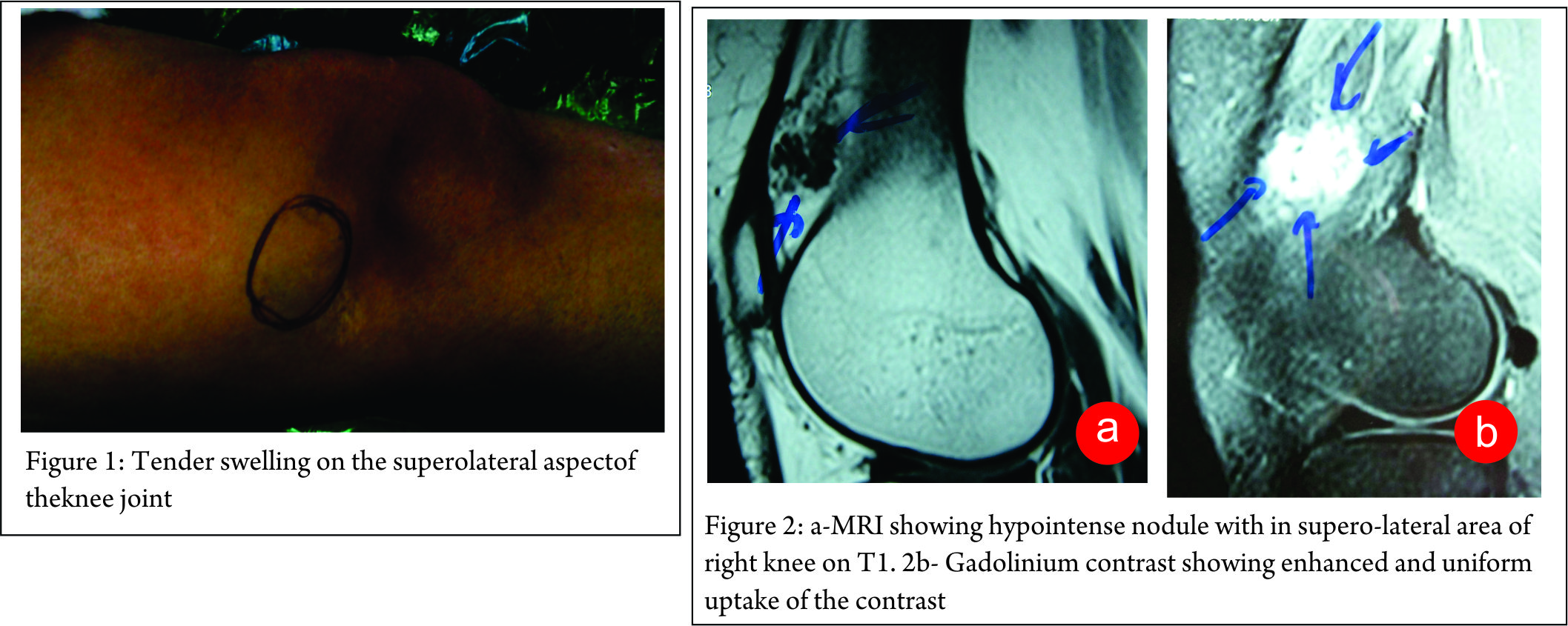
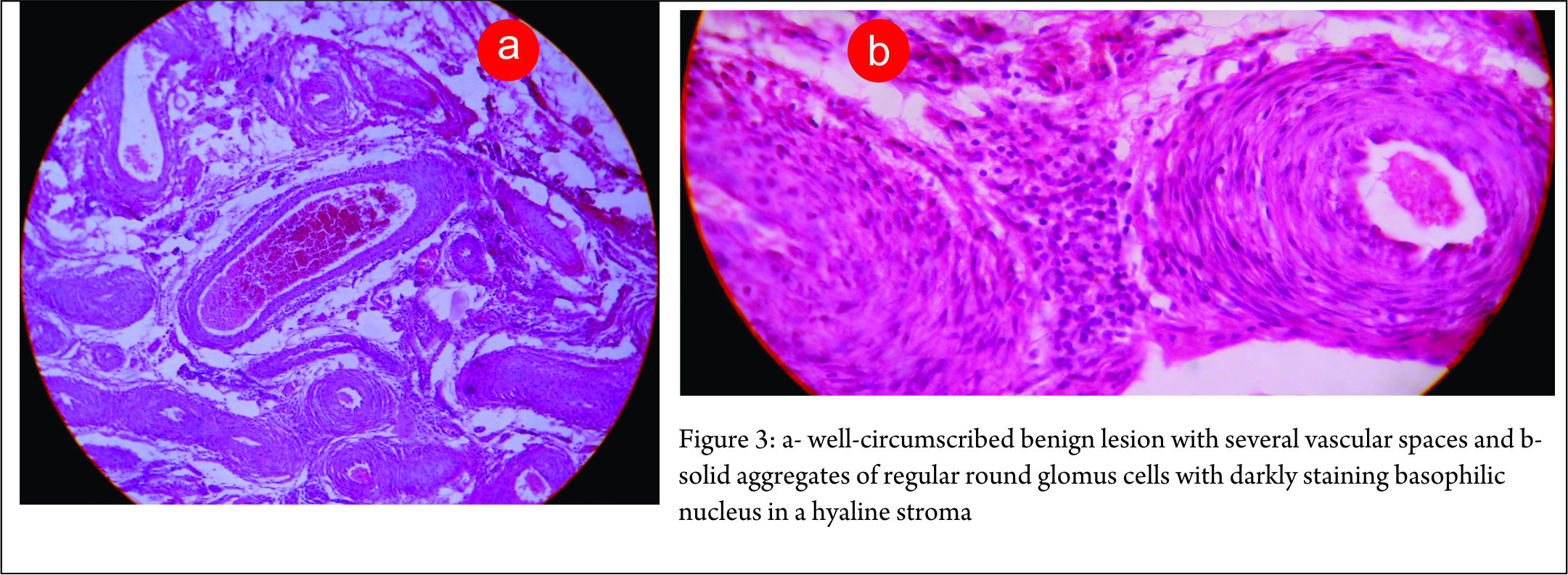
MRI revealed a hypointense nodule with in supero-lateral area of right knee on T1(Fig 2a). Gadolinium contrast showing enhanced and uniform uptake of the contrast (Fig. 2b). This confirmed the vascular nature of the lesion. The authors had earlier treated a similar case of GT of the knee joint and thus a high index of suspicion was present for GT. Excision biopsy was planned for the lesion. Open mini- excision biopsy of the lesion was preferred over arthroscopic shaving so that the lesion could be obtained in toto. The discrete lesion was found to be arising from the capsule of the suprapatellar region of the right knee and was fully excised. The patient had a miraculous recovery from the pain and unusual behaviour pattern. Histological examination revealed a well-circumscribed benign lesion with several vascular spaces (Fig. 3a) and solid aggregates of regular round glomus cells with darkly staining basophilic nucleus in a hyaline stroma.(Fig. 3b). On follow up the patient was completely relieved of all her symptoms. A consent for publication was taken before submitting the case report
Discussion
Histologically GT arises from glomus bodies that are specialised form of arteriovenous anastomosis involved in temperature regulation. Structurally plump endothelial cells line a centrally coiled canal which is surrounded by longitudinal and circular muscle fibres containing rounded epithelial appearing glomus cells (glomocytes) [1,2]. Histologically, GT are divided into 3 subtypes: The classical glomus tumour, glomangiomas and glomangiomyomas, the last being least common. Rarely, glomus tumours may have a malignant potential [3].
Though GT occur more commonly on digits below the nails, they may appear in other anatomical areas. Cutaneous lesions appear as small bluish-red tender nodules in the dermis or sub dermal skin. Pinpoint exquisite tenderness is characteristic. Pain from GT is so severe that at times a patient may even demand an amputation of the limb. The symptoms are generally worse in winter. Extra-digital GT commonly get misdiagnosed for a significant time period before the final diagnosis.4,5,6 In our case too there was a delay of more than a year in diagnosis. GT around the knee are reported infrequently [2,4-22]. In a review of cases GT of mayo clinic, tumors around the knee were 17.8% of all the cases of extradigital GT [2]. The structures around the knee that may be involved can be varied and GT is reported to arise from patellar ligament [9,22], quadriceps muscle [10], vastus lateralis [11], hoffa’s fat pad [13-18], plica synovialis [17]. In our case the lesion was arising from the joint capsule and did not involve muscles or tendons.
We had a very high index of suspicion of GT because of our earlier experience in treating such patients of GT along the knee joint. Often the tumour may not appear for a long time after the pain has begun [23] or may be neglected by the patient [8] or delayed diagnosed [6]. In our case the patient had taken medications from multiple consultants and presented to us with no specific diagnosis. According to Shugart et al, “almost diagnostic is the fact that the patient is reluctant, and often refuses palpation during examination [24]. In our case there was tenderness on deep palpation on complete flexion. This may be because the lesion was deep seated in the capsule and was covered laterally by vastus musculature. The clinical diagnosis needs to be confirmed with MRI and histopathology of the excised tissue. It is important to diagnose glomus tumour because the condition is potentially curable by surgical excision [2,3,4,5]. It however remains intriguing as to why a glomus appeared at this uncommon location.
In conclusion, intractable knee pain with focal exquisite tenderness may be due to glomus tumour and should be suspected early to minimize painful endurance by the patient.
References
1. GombosZ, ZhangPJ. Glomus tumor. Arch Pathol Lab Med 2008;132:1448-52.
2. Schiefer TK, Parker WL, Anakwenze OA, Amadio PC, Inwards CY, Spinner RJ. Extradigital glomus tumors: a 20-year experience. Mayo Clin Proc. 2006 Oct;81(10):1337-44
3. Hiruta N, Kameda N, Tokudome T, Tsuchiya K, Nonaka H, Hatori T, Akima M, Miura M. Malignant glomus tumor: a case report and review of the literature. Am J Surg Pathol. 1997 Sep;21(9):1096-103..
4. Clark ML, O’Hara C, Dobson PJ, Smith AL. Glomus tumour and knee pain: a report of four cases. Knee. 2009; 16: 231-4.
5. Puchala M, Kruczynski J, Szukalski J, Lianeri M. Glomangioma as a rare cause of knee pain. J Bone Joint Surg Am. 2008; 90: 2505-8.
6. Panagiotopoulos E, Maraziotis T, Karageorgos A, Dimopoulos P, Koumoundourou D. A twenty-year delay in diagnosing a glomus knee tumor. Orthopedics. 2006 May;29(5):451-2.
7. Caughey DE, Highton TC. Glomus tumour of the knee. Report of a case. J Bone Joint Surg Br. 1966 Feb;48(1):134-7.
8. Davenport D, Colaco HB, Edwards MR. The 30-year wait for treatment of an acutely painful knee. BMJ Case Rep. 2014 Sep 29;2014.
9.Mabit C, Pecout C, Araud JP. Glomus tumour in the patellar ligament: A case report. J Bone Joint Surg [Am] 1995; 77: 140-141.
10.Negri G, Schulte M, Mohr W. Glomus tumour with diffuse infiltration of the quadriceps muscle: A case report. Hum Path 1997; 28: 750-752.
11.Amillo S, Arriola FJ, Munoz, G. Extradigital glomus tumour causing thigh pain. J Bone Joint Surg [Br] 1997; 79B: 104-106.
12.Oztekin HH. Popliteal glomangioma mimicking baker’s cyst in a 9-year-old child: an unusual location of a glomus tumour. Arthroscopy 2003; 19(7); 1-5.
13.Hardy P, Muller GP, Got C. Glomus tumour of the fat pad. Arthroscopy 1998; 14: 325-328.
14.Waseem S, Jari S, Paton R. Glomus tumour, a rare cause of knee pain: a case report. Knee 2002; 9:161-163.
15. Clark ML, O’Hara C, Dobson PJ, Smith AL. Glomus tumor and knee pain: a report of four cases. Knee. 2009 Jun;16(3):231-4.
16. Gholve PA, Hosalkar HS, Finstein JL, Lackman RD, Fox EJ. Popliteal mass with knee pain in a 57-year-old woman. Clin Orthop Relat Res. 2007 Apr;457:253-9.
17. Kato S, Fujii H, Yoshida A, Hinoki S. Glomus tumor beneath the plica synovialis in the knee: a case report. Knee. 2007 Mar;14(2):164-6.
18. Prabhakar S, Dhillon MS, Vasishtha RK, Bali K. Glomus tumor of Hoffa’s fat pad and its management by arthroscopic excision. Clin Orthop Surg. 2013 Dec;5(4):334-7.
19. Gonçalves R, Lopes A, Júlio C, Durão C, de Mello RA. Knee glomangioma: a rare location for a glomus tumor. Rare Tumors. 2014 Dec 18;6(4):5588.
20. Sraj SA, Khoury NJ, Afeiche NE, Abdelnoor J. Thigh pain of 5 years’ duration in a 48-year-old man. Clin Orthop Relat Res. 2008 Sep;466(9):2291-5.
21. Okahashi K, Sugimoto K, Iwai M, Kaneko K, Samma M, Fujisawa Y, Takakura Y. Glomus tumor of the lateral aspect of the knee joint. Arch Orthop Trauma Surg. 2004 Nov;124(9):636-8.
22. Akgün RC, Güler UÖ, Onay U. A glomus tumor anterior to the patellar tendon: a case report. Acta Orthop Traumatol Turc. 2010;44(3):250-3.
23. King ESJ. Glomus Tumour. Australian and New Zealand Journal of Surgery, 1954:23(4); 280-295.
24. Shugart RR, Soule EH, Johnson EW. Glomus tumor. Surgery, Gynecology & Obstetrics. 1963;117:334–340.
| How to Cite this article: Kulkarni UM, Zavar V, Sankalecha S, Kulkarni A. Intractable Knee pain….it could be Glomus! Journal of Bone and Soft Tissue Tumors May-Aug 2015; 1(1):48-50. |
 Dr.Umesh M Kulkarni |
 Dr.Vijay Zavar |
 Dr.Sudhir Sankalecha |
 Dr.Ameya Kulkarni |
(Abstract) (Full Text HTML) (Download PDF)
