Chemotherapy in Osteosarcoma: Current Strategies
Volume 2 | Issue 1 | Jan-Apr 2016 | Page 27-32 | Sandeep Jain, Gauri Kapoor.
Authers: Sandeep Jain[1], Gauri Kapoor[1]
[1]Department of Pediatric Hematology and Oncology, Rajiv Gandhi Cancer Institute & Research Centre, Delhi.
Address of Correspondence
Dr. Gauri Kapoor MD, PhD
Director Department of Pediatric Hematology and Oncology,
Rajiv Gandhi Cancer Institute & Research Centre, Delhi.
Email: kapoor.gauri@gmail.com
Abstract
Incorporation of chemotherapy to multi-modality management of high grade osteosarcoma has led to remarkable improvement in survival rates. Its use in the neoadjuvant setting is now accepted as standard of care and has the added advantage of providing important information on histologic response. Survival rates for non-metastatic disease are nearly 70%. Outcome of patients with poor histological response and those with metastatic and recurrent disease continues to be unsatisfactory and an ongoing challenge. Therefore, there is a need to develop novel agents and biologically driven strategies to target these disease subgroups. The current review focusses on evolution of chemotherapy, controversies in its use and current standard of care for osteosarcoma.
Keywords: Osteosarcoma, chemotherapy, neoadjuvant chemotherapy.
Introduction
Osteosarcoma is the most common primary malignant bone tumor in children and adolescents accounting for 4% of all pediatric malignancies. Approximately 20% of children present with metastatic disease at diagnosis and it remains, unquestionably the most important factor affecting long term survival. Prior to 1970, the prognosis of patients with osteosarcoma was dismal, with a 10–20 % overall survival despite being treated with radical surgeries [1-3]. Outcome of patients with osteosarcoma has improved in the past three decades with the addition of effective systemic polychemotherapy and advances in surgical resection. These have led to improvements in overall survival of patients with localized disease to the tune of 70% [4-5]. Various well coordinated systemic trials by different co-operative groups in North America and Europe have identified high-dose methotrexate (HD-MTX), cisplatin, doxorubicin, ifosfamide and etoposide as active cytotoxic agents and combinations of these drugs make up the cornerstone of treatment. Chemotherapy not only takes care of micrometastatic disease at diagnosis but also facilitates limb salvage surgery. The choice of regimen and optimal schedule of chemotherapy is somewhat controversial. In this review we focus on evolution of chemotherapy, controversies in chemotherapy use and current standard of care.
Evolution of chemotherapy
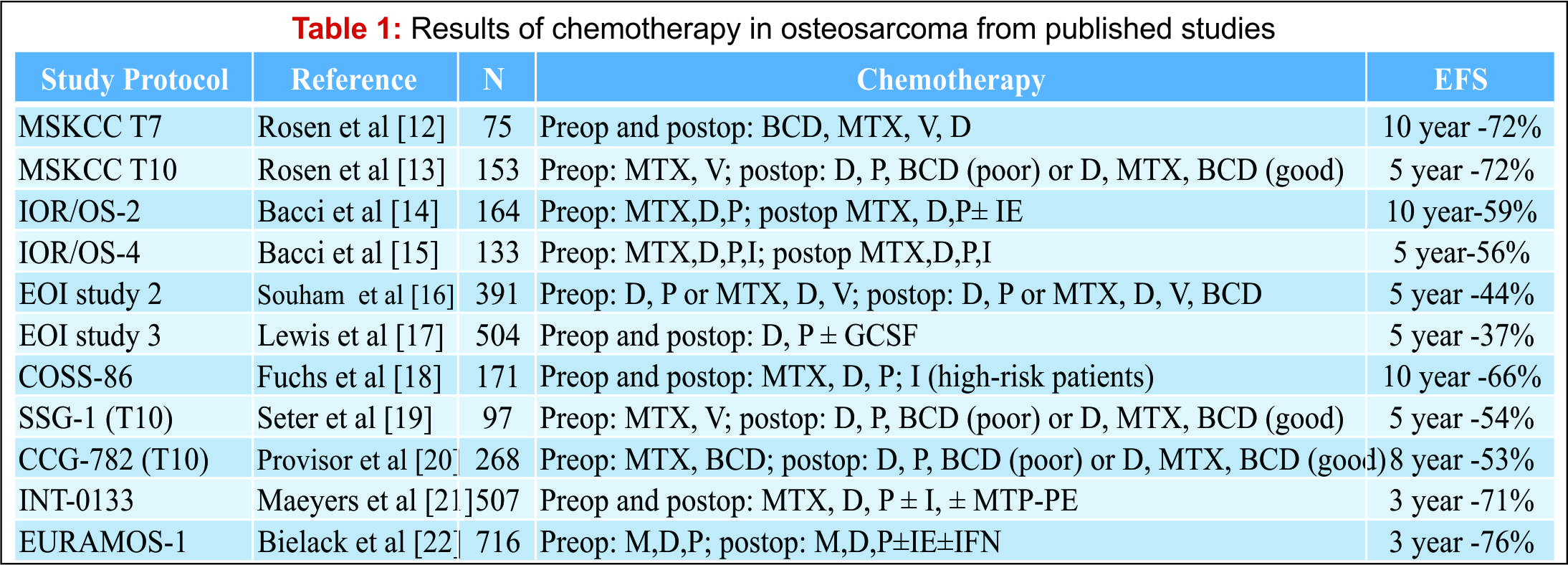
Before the introduction of chemotherapy, the outcome of patients with osteosarcoma was only 15-20%, despite adequate local control. Most patients succumbed to metastatic lung disease. These findings led to the conclusion that patients with osteosarcoma have microscopic metastatic disease at the time of diagnosis and this prompted investigators to identify active agents to target it. Initial studies to demonstrate chemosensitivity of osteosarcoma were done in the early 1970s by Sutow et al [6]. He developed a regimen called “Conpadri”which included cyclophosphamide, Oncovin (vincristine), doxorubicin (adriamycin), and L-phenylalaninemustard. Later on with the inclusion of HD-MTX, the acronym was changed to “Compadri’ [6-7]. These regimes were the first rational attempt at confirming the role of adjuvant combination chemotherapy using drugs with non-overlapping toxicities in osteosarcoma. Compadri I–III yielded a 41% 18-month disease-free survival [8]. These results suggested that addition of chemotherapy improved survival in patients with osteosarcoma. However, in the absence of randomized trials, it was not clear, to what extent improvement in surgical techniques and radiological studies contributed to achieving these results. These observations were further supported by the first randomized trial from Mayo clinic wherein patients were randomized to receive adjuvant vincristine and HD-MTX versus surgery alone[9]. This trial did not show any difference between the two arms. All these concerns were put to rest by two subsequent randomized controlled trials from North America that clearly established the survival benefit of adjuvant chemotherapy. In both these trials patients receiving no adjuvant treatment had a 2 year event free survival of just 20% compared to 66% and 55% in patients who received adjuvant chemotherapy [10-11]. These trials also established adriamycin, cisplatin, HD-MTX and alkylating drugs like ifosfamide and etoposide as active agents in the treatment of osteosarcoma. The various trials showing benefit of chemotherapy in osteosarcoma are listed in Table 1[12-22].
Role of neoadjuvant chemotherapy
The concept of neoadjuvant chemotherapy (NACT) was first introduced at Memorial Sloan-Kettering Cancer Center (MSKCC) in their T-10 protocol [23]. Preoperative chemotherapy was administered in an effort to increase the number of patients who could undergo limb salvage as the surgeons needed time to order the prosthetic devices. Administration of NACT also had the theoretical advantage of treating presumed microscopic metastatic disease. The outcome of the T-10 trial was similar to that of the Multi Institutional Osteosarcoma Study (MIOS), with a 65% survival rate at 5 years. Importantly, the results of this trial laid the foundation for the subsequent important association between histologic necrosis and prognosis. However, there were concerns regarding the impact of delayed surgery among patients with chemo-resistant disease as well as the probability of development of resistant clone in those with high volume disease. To answer this concern Pediatric Oncology Group conducted a randomized clinical trial (POG 8651) between 1986 and 1993, comparing NACT with adjuvant chemotherapy. This trial compared immediate surgery followed by postoperative adjuvant chemotherapy with 10 weeks of the NACT (same drugs) followed by surgery in 100 patients under the age of 30 years with non-metastatic,high grade osteosarcoma. Chemotherapy consisted of alternating courses of HD-MTX with leucovorin rescue, cisplatin, doxorubicin, and bleomycin, cyclophosphamide,dactinomycin (BCD). The five-year relapse-free survival rates were similar between the two groups, 65% versus 61% for adjuvant and neoadjuvant arms respectively. There was also no difference in the number of patients who underwent limb salvage procedures (55% and 50 % for immediate and delayed surgery, respectively) [24]. On the basis of these results, the use of preoperative chemotherapy has become standard of care, given its advantages, as it allows sufficient time for surgical planning, potentially facilitates tumor removal, and permits evaluation of response to therapy. Several investigators in single and multi-institutional studies in the United States and across Europe, support this general strategy [13,14,16,18].
Histological response to chemotherapy
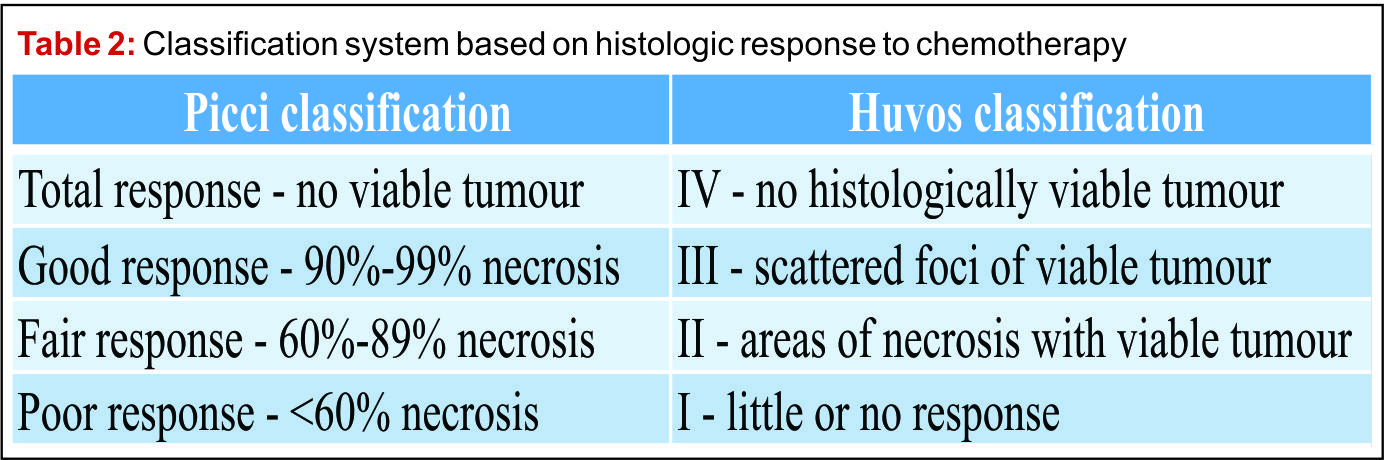
Most trials reveal that patients with greater than 90% necrosis following NACT have significantly better event free survival (EFS) compared to those with less than 90% necrosis. Several grading systems have been developed for assessing the effect of preoperative chemotherapy on the tumor. The two most commonly used classification systems are the Picci and Huvos classifications[Table 2]. The Institute of Rizzoli (IOR) reviewed data on localized extremity osteosarcoma in more than 1000 patients over the 19-year period from 1983 to 2002 [25]. Fifty-nine percent of all patients had good response to chemotherapy (Picci), and had a 5-year survival of 76%, compared to 56% for poor responders. The Cooperative Osteosarcoma Study group (COSS) database analyzed 1,700 patients between 1980 and 1998 that included all sites, ages, and presence or absence of metastases [26]. The data revealed that 55.6% of patients had good response to therapy. The 5-year survival rate for good and poor responders was 77.8% and 55.5% respectively. The European Osteosarcoma Intergroup (EOI) analyzed data of two consecutive studies between 1983 and 1986 and 1986 and 1991 [27]. A total of 570 patients were analyzed in the report. This analysis is notable for several differences compared to the COSS and IOR analyses. Only 28% of patients had a good histologic response, whereas 72% of patients had a poor histologic response. Their 5-year survival rate was 75% and 45% respectively. Interestingly, many of the patients included in the analysis did not receive HD-MTX as they were randomized to receive either doxorubicin and cisplatin or more intensive therapy including doxorubicin and HD-MTX. This data clearly established that histological response to chemotherapy is an important prognostic factor.
Intensification of neoadjuvant and adjuvant chemotherapy
As it became clear that the degree of histological necrosis after pre-operative chemotherapy predicts survival, efforts were directed to intensify chemotherapy so as to achieve maximum therapeutic response. This strategy of preoperative chemotherapy intensification has been tested in COSS-86 and MSKCC T-12 study [14,28]. Although this strategy resulted in increased proportion of good responders achieving >90% necrosis, it did not translate into improved overall survival (OS) or EFS rates. Till date only INT-0133 study has shown benefit of NACT intensification [19]. The next group of trials focused to alter or intensify chemotherapy for patients with sub-optimal response to preoperative chemotherapy. In the early 1980s at Memorial Sloan-Kettering Cancer Center, poor responders had cisplatin substituted for HD-MTX in addition to continuing BCD (bleomycin, cyclophosphamide, and dactinomycin) and doxorubicin [13]. Survival of patients with intensified adjuvant treatment was similar to others. Several other reports have also failed to demonstrate benefit of intensification of therapy for poor responders[20,29]. Thus, till date it has not been possible to improve the outcome of poor responders by altering postoperative chemotherapy. An explanation for this may be that the NACT response is a surrogate measure of chemo-sensitivity of tumor and an inherently biologic unresponsive tumor is not modifiable by currently available therapies.
Role of intra-arterial chemotherapy
The intra-arterial route was introduced in an attempt to enhance the efficacy of drugs by increasing the local concentration of chemotherapy. Alkylating agents like ifosfamide and cyclophosphamide could not be used as they required phosphorylation in liver for activation. Doxorubicin was not a suitable agent as it is associated with skin and subcutaneous necrosis. MTX achieved high tumoricidal concentrations intra-arterially but similar concentrations could also be attained via the intravenous route. Intra-arterial cisplatin was therefore, selected and found to be highly effective. Response rates with the intra-arterial route were better when compared to the intravenous route[30]. It has been used extensively at the MD Anderson Cancer Center in the TIOS pediatric trials. It was highly effective in patients with pathological fractures and neurovascular involvement. Unfortunately, intra-arterial route is labor intensive and requires general anaesthesia or conscious sedation in a radiological suite. It also requires intensive monitoring of the distal arterial vascular status during and after the infusion. Moreover, similar results could be achieved with multiple courses of combination chemotherapy administered by the intravenous route over a more prolonged period. Therefore, intra-arterial route is generally not preferred.
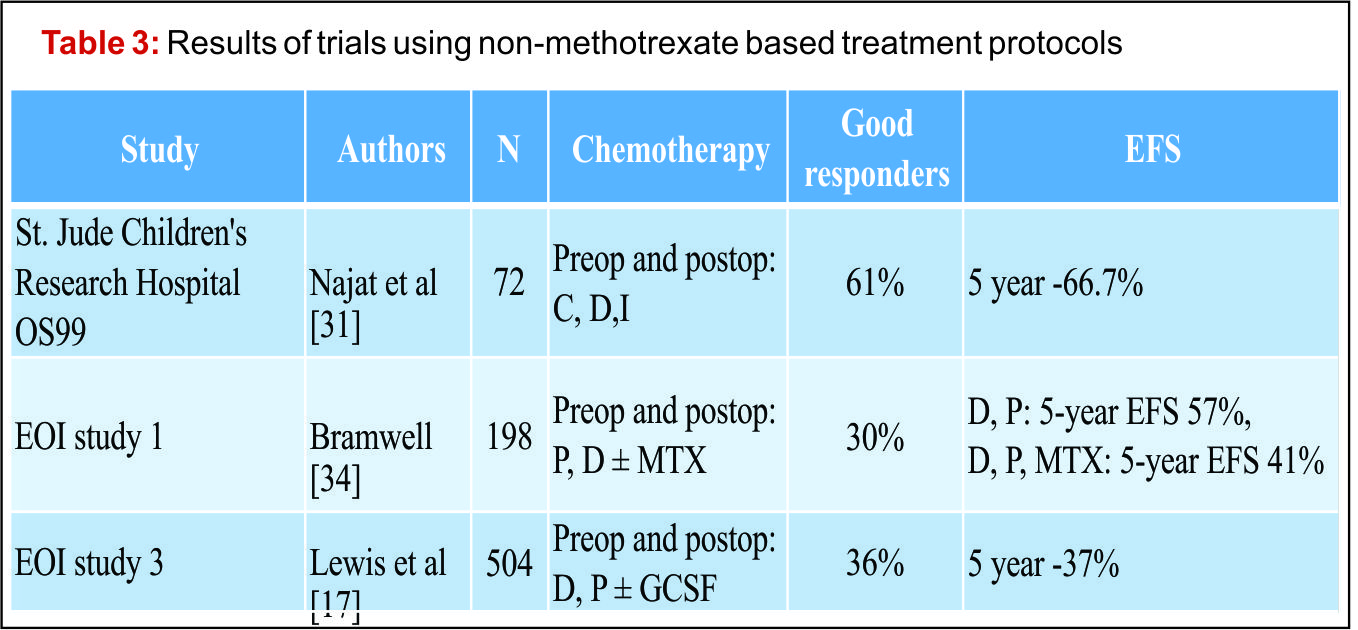
High Dose Methotrexate
High dose methotrexate is one of the oldest drugs used in the treatment of osteosarcoma. It is generally administered over 4-6 hours and requires aggressive hydration, leucovorin rescue, serum level monitoring and adequate infrastructure to safeguard delivery and manage toxicity. Moreover, it adds substantially to the overall cost of treatment. In addition, there are no randomized studies to compare the efficacy of higher versus intermediate doses of HD-MTX plus doxorubicin and cisplatin versus doxorubicin/cisplatin alone. Furthermore, investigators at St. Jude Children’s Research Hospital have demonstrated good outcomes with five-year EFS and OS of 66% and 75% respectively with non-methotrexate-containing chemotherapy regimen consisting of carboplatin, ifosfamide and doxorubicin [31]. All of this has led to considerable controversy regarding the optimum role of HD-MTX. Methotrexate is the only active agent that has been subjected to a comparative trial of efficacy with another active agent i.e. cisplatin. Compared to 5-20% survival of historical controls in pre-chemotherapy era, HD-MTX increased survival to 40% – 60% as a single agent. When combined with other active agents like cisplatin and doxorubicin the long term survival of 65% – 75% was reported [12-15]. Many studies have shown a favorable correlation between peak serum levels and outcome [19,32-33]. Therefore, optimum doses and administration schedule is crucial to derive optimum benefit from HD-MTX therapy. Chemotherapy regimes devoid of HD-MTX were considered, among the “major poor prognostic factors” in the treatment of osteosarcoma by Graf et al. [33]. Despite the absence of randomized trials evaluating osteosarcoma treatment with and without HD-MTX, it is generally acknowledged that methotrexate is a standard component of almost all contemporary osteosarcoma protocols in children and adolescents.
Current standard of care for patients with osteosarcoma
It is well established that chemotherapy is an integral component of osteosarcoma treatment and is essential in addition to local surgery in order to achieve a reasonable expectation of cure. Therefore, optimum treatment for osteosarcoma demands a multidisciplinary strategy. The treatment generally consists of three stages: initial cytoreduction with chemotherapy to eradicate micro metastatic disease and facilitate effective local control measures with wide negative margins; and consolidation therapy for eradication of occult residual disease to reduce the likelihood of tumor recurrence. Importantly, NACT not only helps to achieve optimal cytoreduction in facilitating limb salvage procedures but also provides a chance to assess the histologic response to chemotherapy. Most treatment protocols include cisplatin, doxorubicin and HD-MTX with or without ifosfamide plus etoposide(IE). In the recently concluded EURAMOS study, all patients received NACT: 2 blocks of MAP (methotrexate, doxorubicin and cisplatin) chemotherapy for 10 weeks followed by surgery (wide excision). Surgical excision of tumor with oncologically safe margins was the best means of local control. Post surgery, poor responders were randomized to receive MAP for 28 weeks with or without IE. All good responders continued on MAP for 28 weeks and then were randomized to no further therapy and maintenance therapy with pegylated interferon. This is the largest international trial in the history of osteosarcoma treatment and its results show that intensification of adjuvant chemotherapy by addition of IE in poor responders did not improve survival. Furthermore, in good responders addition of pegylated interferon maintenance was not useful [22]. Schema of this treatment is shown in [Figure 1] and most of the study groups endorse this strategy as current standard of care.

Non-methotrexate based chemotherapy for countries with limited resources
There is paucity of published data on osteosarcoma from India. Historically, the role of high dose methotrexate in the treatment of osteosarcoma has always been debatable. From the practical perspective, it requires rigorous pharmacokinetic monitoring and often the infrastructure required for monitoring is not available in many centers with limited resources. Therefore, most of the centers in India use cispaltin, doxorubicin and ifosfamide based chemotherapy. Pathak et al have reported relapse-free survival was 72% nonmetastatic osteogenic sarcoma of the extremities using cisplatin and doxorubicin as adjuvant therapy [35]. Recently, results from a single center study from India have revealed 2yr progression free survival of 70 % for patients with non-metastatic osteosarcoma [36]. In light of these results use of non methotrexate based therapy in resource constraint setting seems justified. In addition, it is desirable to focus on developing infrastructure to provide limb salvage procedures and direct resources to develop indigenous affordable prosthesis.
Treatment of relapsed osteosarcoma
Treatment of relapsed osteosarcoma has not been tested in randomized clinical trials, and thus, there is no single standard approach. Prognosis of patients with relapse depends on duration of off therapy and site of relapse. In a large database of 565 osteosarcoma patients who relapsed after being treated with one of three different NACT protocols within the European Osteosarcoma Intergroup, five year survival post relapse in those whose disease recurred after two years versus within two years of randomization was 35 versus 14 percent, respectively[37]. There is no reasonable chance of cure without complete surgical resection of all sites of disease. Choice of chemotherapy depends on agents used in front line therapy. In most of contemporary studies, most of the patients receive cisplatin and doxorubicin in front line therapy. Therefore, ifosfamide, etoposide and HD-MTX are the most commonly used drugs in relapse setting. In general, patients should be treated with any of the four most active agents that were not included in front line therapy. The use of high-dose chemotherapy with autologous hematopoietic stem cell rescue has been applied to salvage therapy. However, at least two small pilot studies failed to demonstrate significant advantage of standard salvage therapy approaches [38-39].
Newer therapies
There has been significant progress in the management of patients with osteosarcoma from 1970 to 1990. However, thereafter, progress has been stalled due to limited options available for patients with poor histologic response and those with metastatic and recurrent disease. It is clear that intensification of available chemotherapeutic agents has not translated into survival benefit for these group of patients and novel agents are required. Some of the agents being tested include mTOR inhibitor (ridaforolimus), inhibitors of insulin-like growth factor I receptor, tyrosine kinase inhibitor (sorafenib), microtubule inhibitor (oferibulin), human monoclonal antibody against RANKL (Denosumab) and anti-disialoganglioside antibody (theuseofan) [40-44]. Some of these agents have demonstrated promising results in preclinical data and may offer a potential role in adjuvant therapy in the future.
Acute toxicities and Late Effects
The most frequent acute toxicities due to chemotherapy are infections secondary to myelosuppression and mucositis. Renal dysfunction may lead to hypomagnesemia and other electrolyte abnormalities from tubular and glomerular damage induced by ifosfamide and cisplatin respectively. Ototoxicity from cisplatin and cardiac dysfunction related to anthracyclines are the other commonly observed side effects. Late effects in osteosarcoma may be attributed to local therapy i.e. surgery or to systemic chemotherapy. Those related to chemotherapy are usually agent specific. Doxorubicin is known to cause chronic cardiomyopathy which is dependent on the total cumulative dose. Longhi et al reported 2% incidence of symptomatic cardiomyoathy at a median follow up of 10 years [45]. In general, cumulative dose of doxorubicin is usually limited to less than 450 mg/m2. Anthracycline and alkylating agents may also result in second malignant neoplasm (SMN). The same authors report a 10-year and 20-year cumulative incidence of SMN of 4.9% and 6.1% respectively in osteosarcoma survivors. The alkylating agent, ifosfamide is associated with infertility, especially male infertility, so sperm cryopreservation should be offered to postpubertal boys if treatment plan includes alkylating agents. In addition, ifosfamide can cause a persistent renal tubular electrolyte loss and, less commonly, a decrease in glomerular function, in a dose-dependent fashion.
Conclusion
Inclusion of chemotherapy in the multimodality treatment of osteosarcoma has undoubtedly improved survival from a dismal 20% to the present 60%. NACT has enabled limb salvage rates to the tune of 90-95% in most advanced centers. Outcome of patients with poor histological response and those with metastatic and recurrent disease continues to be unsatisfactory and an ongoing challenge. Therefore, there is a need to develop novel agents and biologically driven strategies to target these disease subgroups.
References
1. Francis K, Worcester JJ. Radical resection for tumors of the shoulder with preservation of a functional extremity. J Bone Joint Surg Am 1962;44:1423
2. Marcove RC, Miké V, Hajek JV, Levin AG, Hutter RV. Osteogenic sarcoma under the age of twenty-one: A review of one hundred and forty-five operative cases. J Bone Joint Surg Am 1970;52(3):411
3. Friedman MA, Carter SK. The therapy of osteogenic sarcoma: current status and thoughts for the future. J SurgOncol, 1972;4:482–510
4. Link MP, Gebhardt MC, Meyers PA. Osteosarcoma. In: Pizzo A, Poplack G (eds), Principles and Practice of Pediatric Oncology, 4th edition, Philadelphia: Lippincott Williams and Wilkins. 2002;1051–89.
5. Meyers P, Osteosarcoma. In: Pappo A (ed.), Pediatric Bone and Soft Tissue Sarcomas, Berlin: Springer-Verlag. 2006;219–33
6. Sutow WW. Combination Chemotherapy with Adria- mycin (NSC-123127) in Primary Treatment of Osteogen- icsarcoma (Part III) Cancer Chemotherapy Reports. 1975;6: 315-317
7. Sutow WW, Gehan EA, Dyment PC. Multi- Drug Adjuvant Chemotherapy in Osteosarcoma. Interim Report of the Southwest Oncology Group Studies. Cancer Chemotherapy Reports 1962; 62:265-269
8. Herson J, Sutow WW, Elder K. Adjuvant chemotherapy in nonmetastatic osteosarcoma: a Southwest Oncology Group study. Medical and Pediatric Oncology 1980;8:343– 352
9. Edmonson JH, Creagan ET, Gilchrist GS. Phase II study of high-dose methotrexate in patients with unresectable metastatic osteosarcoma. Cancer Treat Rep 1981; 65:538
10. Link MP, Goorin AM, Miser AW et al. The effect of adjuvant chemotherapy on relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986; 314: 1600-1606
11. Eilber F, Giuliano A, Eckardt J, Patterson K, Moseley S, Goodnight J. Adjuvant chemotherapy for osteosarcoma: a randomized prospective trial. J.Clin.Oncol 1987; 5: 21-26.
12. Rosen G, Nirenberg A, Caparros B et al. Osteogenic sarcoma: eight-percent, three-year, disease-free survival with combination chemotherapy (T-7). Natl Cancer Inst Monogr 1981;56:213-20
13. Rosen G, Caparros B, Huvos AG et al Preoperative chemotherapy for osteogenic sarcoma: selection of postoperative adjuvant chemotherapy based on the response of the primary tumor to preoperative chemotherapy Cancer. 1982;49:1221-30
14. Bacci G, Ferrari S, Bertoni F, et al. Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the istitutoortopedicorizzoli according to the istitutoortopedicorizzoli/osteosarcoma-2 protocol: an updated report. J ClinOncol 2000;18:4016–27
15. Bacci G, Briccoli A, Ferrari S, et al. Neoadjuvant chemotherapy for osteosarcoma of the extremity: long-term results of the Rizzoli’s 4th protocol. Eur J Cancer 2001;37:2030–9
16. Souhami RL, Craft AW, EijkenJWvd, et al. Randomised trial of two regimens of chemotherapy in operable osteosarcoma: a study of the European Osteosarcoma Intergroup. Lancet 1997;350:911–7
17. Lewis IJ, Nooij MA, Whelan J, et al. Improvement in histologic response but not survival in osteosarcoma patients treated with intensified chemotherapy: a randomized phase III trial of the European Osteosarcoma Intergroup. J Natl Cancer Inst 2007;99:112–28
18. Fuchs N, Bielack SS, Epler D, et al. Long-term results of the co-operative German-Austrian-Swiss osteosarcoma study group’s protocol COSS-86 of intensive multidrug chemotherapy and surgery for osteosarcoma of the limbs. Ann Oncol 1998;9:893–9
19. Seter G, Alvegård TA, Elomaa I et al. Treatment of osteosarcoma of the extremities with the T-10 protocol, with emphasis on the effects of preoperative chemotherapy with single-agent high-dose methotrexate: a Scandinavian Sarcoma Group study. J ClinOncol 1991;9:1766-75
20. Provisor AJ, Ettinger LJ, Nachman JB, et al. Treatment of nonmetastatic osteosarcoma of the extremity with preoperative and postoperative chemotherapy: a report from the Children’s Cancer Group. J ClinOncol 1997;15:76
21. Meyers PA, Schwartz CL, Krailo M et al. Osteosarcoma: a randomized, prospective trial of the addition of ifosfamide and/or muramyltripeptide to cisplatin, doxorubicin, and high-dose methotrexate. J ClinOncol 2005;23(9):2004-11
22. Bielack SS, Smeland S, Whelan JS, et al. Methotrexate, doxorubicin, and cisplatin (MAP) plus maintenance interferon alfa-2b versus MAP alone in patients with resectable high-grade osteosarcoma and good histologic response to preoperative MAP: First results of the EURAMOS-1 good response randomized controlled trial. J ClinOncol 33:2279-2287, 2015
23. Rosen G, Marcove RC, Caparros B, et al. Primary osteogenic sarcoma: The rationale for preoperative chemotherapy and delayed surgery. Cancer 43:2163-2177, 1979
24. Goorin AM, Schwartzentruber DJ, Devidas M, et al. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: Pediatric Oncology Group Study POG-8651. J ClinOncol 2003;21:1574–80
25. Bacci G, Bertoni F, Longhi A, et al. Neoadjuvant chemotherapy for high-grade central osteosarcoma of the extremity: Histologic response to preoperative chemotherapy correlates with histologic subtype of the tumor. Cancer 2003;97):3068
26. Bielack SS, Nishida Y, Nakashima H, Shimoyama Y, Nakamura S, Ishiguro N. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J ClinOncol 2002;20:77
27. Hauben EI, Weeden S, Pringle J, Van Marck EA, Hogendoorn PC. Does the histological subtype of high-grade central osteosarcoma influence the response to treatment with chemotherapy and does it affect overall survival? A study on 570 patients of two consecutive trials of the European Osteosarcoma Intergroup. Eur J Cancer 2002;38:1218
28. Meyers PA, Gorlick R, Heller G, et al. Intensification of preoperative chemotherapy for osteogenic sarcoma: results of the Memorial Sloan-Kettering (T12) protocol. J ClinOncol 1998;16:2452–8
29. Winkler K, Beron G, Delling G, et al. Neoadjuvant chemotherapy of osteosarcoma: results of a randomized cooperative trial (COSS-82) with salvage chemotherapy based on histological tumor response. J ClinOncol 1988;6:329
30. Bielack S, Ertman R, Looft G, Purfürst C, Delling G, Winkler K, Landbeck G. Platinum disposition after intraarterial and intravenous infusion of cisplatinum for osteosarcoma. Cancer ChemotherPharmacol 1988;24:376-80
31. Daw NC, Neel MD, Rao BN, et al. Frontline treatment of localized osteosarcoma without methotrexate: results of the St. Jude Children’s Research Hospital OS99 trial. Cancer 2011; 117:2770
32. Delepine N, Delepine G, Jasmin C, et al. Importance of age and methotrexate dosage: prognosis in children and young adults with high-grade osteosarcomas. Biomed Pharmacother 1988; 42:257
33. Graf N, Winkler K, Betlemovic M, et al. Methotrexate pharmacokinetics and prognosis in osteosarcoma. J ClinOncol 1994; 12:1443
34. Bramwell VH, Burgers M, Sneath R, et al. A comparison of two short intensive adjuvant chemotherapy regimens in operable osteosarcoma of limbs in children and young adults: the first study of the European Osteosarcoma Intergroup. J ClinOncol. 1992;10:1579–1591
35. Pathak AB, Advani SH, Iyer RS et al. Adjuvant chemotherapy for osteogenic sarcoma of the extremity with sequential adriamycin and cisplatin. J SurgOncol. 1993;52:181-4
36. Bajpai J, Chandrakanth MV, Shetty N et al. s non-HD–MTX based, dose-dense, combination chemotherapy a valid choice in osteosarcoma in developing world? J ClinOncol 2014 ;32:5s, (suppl; abstr 10537)
37. Gelderblom H, Jinks RC, Sydes M, et al. Survival after recurrent osteosarcoma: data from 3 European Osteosarcoma Intergroup (EOI) randomized controlled trials. Eur J Cancer 2011; 47:895
38. Sauerbrey A, Bielack S, Kempf-Bielack B, Zoubek A, Paulussen M, Zintl F. High-dose chemotherapy (HDC) and autologous hematopoietic stem cell transplantation (ASCT) as salvage therapy for relapsed osteosarcoma. Bone Marrow Transplant 2001;27:933
39. Fagioli F, Aglietta M, Tienghi A, et al. High-dose chemotherapy in the treatment of relapsed osteosarcoma: an Italian sarcoma group study. J ClinOncol 2002;20:2150
40. Chawla SP, Staddon AP, Baker LH, et al. Phase II study of the mammalian target of rapamycin inhibitor ridaforolimus in patients with advanced bone and soft tissue sarcomas. J ClinOncol 30:7884, 2012
41. GrignaniG,PalmeriniE,DileoP,etal. Aphase II trial of sorafenib in relapsed and unresectable high-grade osteosarcoma after failure of standard multimodal therapy: An Italian Sarcoma Group study. Ann Oncol 23:508-516, 2012
42. Kolb EA, Gorlick R, Reynolds CP, et al. Initial testing (stage 1) of eribulin, a novel tubulin binding agent, by the pediatric preclinical testing program. Pediatr Blood Cancer 60:1325-1332, 2013
43. Beristain AG, Narala SR, Di Grappa MA, et al. Homotypic RANK signaling differentially regulates proliferation, motility and cell survival in osteosarcoma and mammary epithelial cells. J Cell Sci 125: 943-955, 2012
44. Roth M, Linkowski M, Tarim J, et al. Ganglioside GD2 as a therapeutic target for antibodymediated therapy in patients with osteosarcoma. Cancer 120:548-554, 2014
45. Longhi A, Ferrari S, Tamburini A, et al. Late effects of chemotherapy and radiotherapy in osteosarcoma and Ewing sarcoma patients: the Italian Sarcoma Group Experience (1983-2006). Cancer. 2012;118:5050-5059.
| How to Cite this article:Jain S, Kapoor G. Chemotherapy in Osteosarcoma: Current Strategies. Journal of Bone and Soft Tissue Tumors Jan-Apr 2016;2(1):27-32 . |